Received: March 18, 2014
Accepted: July 23, 2014
Meditterr J Hematol Infect Dis 2014, 6(1): e2014057 doi: 10.4084/MJHID.2014.057
This article is available on PDF format at:

Azza A.G.Tantawy1, Nagham El Bablawy1, Amira A. M Adly1 and Fatma S.E. Ebeid1
1Departments of Pediatrics, Ain Shams University, Cairo, Egypt
| This is an Open Access article distributed under the
terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background: Better
survival of thalassemia patients allowed previously unrecognized renal
complications to emerge.
Objectives: Assess prevalence and early predictors of renal dysfunction in young β-thalassemia major (β-TM) and intermedia (β-TI) patients.Subjects:66 β-TM (group I), 26 β-TI (group II) Egyptian patients and 40 healthy controls. Methods: Clinical assessment and laboratory data including kidney and liver function tests, such as serum ferritin, serum bicarbonate, plasma osmolality and urinary total proteins, microalbuminuria (MAU), N-acetyl-β-D-glucosaminidase (NAG), retinol binding protein (RBP), α-1 microglobulin, bicarbonate, osmolality, creatinine clearance (CrCl), % fractional excretion of bicarbonate (% FE-HCO3). Results: The prevalent renal abnormality was proteinuria (71%), followed by increased urinary level of RBP (69.4%), NAG (58.1%), α-1 microglobulin (54.8%) and microalbuminuria (29%) and also decreased urinary osmolality (58.1%). CrCl was a better assessment of renal function and significantly lowered in thalassemia patients. Tubular dysfunctions were more significant in splenectomized β-TM patients who showed more elevation of NAG and α-1 microglobulin and lower urinary osmolality. NAG, RBP and α-1 microglobulin were negatively correlated with CrCl and positively correlated with serum ferritin and urinary total protein. Z-score analysis for identifying patients with renal dysfunction proved superiority of urine total protein and RBP. Comparative statistics of different frequencies revealed significant difference between the urinary total protein and both MAU and % FE-HCO3. Conclusion: Asymptomatic renal dysfunctions are prevalent in young β-TM and β-TI patients that necessitate regular screening. Urinary total protein and RBP may be cost-effective for early detection. |
Introduction
Improvement of survival in patients with β-thalassemia has allowed
several clinical morbidities to manifest, including renal
complications.[1] Renal dysfunction in these patients
is not fully
understood and seems to be multifactorial; attributed mainly to
long-standing anemia, chronic hypoxia, iron overload and toxicity of
iron chelators.[2]
Evidence of proximal tubular damage is observed in patients with β-TM.
Low-molecular-weight proteinuria is found in almost all patients.
Moreover, several studies report increased urinary excretion of several
markers of proximal tubular damage in a considerable number of patients
with β-TM. including N-acetyl-b-D-glucosaminidase (NAG) and
b2-microglobulin (up to 60%); calcium (approximately 13%), phosphate
and magnesium (about 9%), uric acid (30%–40%), amino acids
(approximately 30%), and malondialdehyde derived from the destruction
of membrane lipids by peroxidation.[3]
Assessment of tubular function involves evaluation of functions of the
both proximal tubule (tubular handling of sodium, glucose, phosphate,
calcium, bicarbonate and aminoacids) and distal tubule (urinary
acidification and concentration).[4] The integrity of
renal tubules can
be examined through urinary measurement of one or more proteins of low
molecular weight (LMW), as α-1 microglobulin (31 KD) and retinol
binding protein (RBP) (22KD).[5] Both these parameters
are freely
filtered through the glomeruli and reabsorbed by proximal convoluted
tubules.[6] Although the enzyme NAG is of high
molecular weight (140
KD), it is considered as a marker of renal tubular function mainly
because it is secreted by tubular epithelium and its measurement has
been undertaken in a variety of diseases associated with renal
injury.[7]
Glomerular integrity can be assessed by measuring the concentration of
urinary protein that is predominantly retained by the healthy
glomerulus. The proteinuria of glomerular origin is an independent risk
factor that strongly predicted those patients at great risk of
progressive loss of renal function.[8]
Early identification of patients, at high risk of developing renal
failure, is of great importance as it may allow specific measures to
delay the progression of renal damage and thus reduce the incidence of
end-stage renal failure and mortality.[9] We aimed to
evaluate the
renal function status in β-TM and β-TI patients through comprehensive
laboratory testing to entail the proper site of the lesion, either
glomerular or tubular and assess prevalence and severity of renal
glomerular and tubular dysfunction, and determine its early predictors.
Subjects
A cross-sectional, case-control study has been performed including
66 patients with β-TM (group I) and 26 β-TI (group II) attending the
Pediatric Hematology Clinic, Ain Shams University. Their diagnoses were
based on hematological parameters and hemoglobin electrophoresis and
were classified into:
[one] Group-I comprised 66 patients with β-TM, aged 2.5 - 13 years
(mean 6.8 ±3.3 years), 42 males and 24 females, they were subdivided
into two subgroups; Group-Ia (splenectomized group) (n°40) Group-Ib
(non-splenectomized group) (n° 26). They received approximately 15 ml
of packed red blood cells per kilogram body weight at each transfusion
every 2-3 weeks interval, to maintain their hemoglobin levels around 8
g/dl.
[two] Group-II comprised 26 patients β-TI, aged 2.5 - 16 years (mean
7.6±4.7 years), 18 males and eight females. They were intermittently
transfused, and their transfusion therapy was initiated mainly for
failure to thrive in childhood, persistent worsening of their anemia,
or development of complications during the course of the disease.
The study also included 40 healthy children, age and sex matched, as
control group (Group-III).
The study was approved by The Medical Ethics Committee of Human
Experimentation of Ain Shams University. Informed consent was obtained
from parents or legal guardians.
Methods
All recruited children were subjected to a detailed history with
emphasis on disease duration, transfusion and chelation history,
splenectomy status and symptoms suggesting renal abnormalities. A
clinical examination stressing on anthropometric measures, and
including echography for abdominal and renal assessment, was conducted
on patients. Furthermore, they were subjected to comprehensive
laboratory investigations including:
1. Hematological assessment included complete blood count (CBC),
hemoglobin analysis with HPLC (high-performance cation exchange liquid
chromatography), and indirect bilirubin dosage, as a marker of
hemolysis.
2. Serum creatinine and blood urea nitrogen (BUN) were classified
according to standard normal ranges for age and sex.[10]
Creatinine
clearance (CrCl) was calculated from 24-h urine specimens using the
standard formula: (U)*(V/P)/(1.73/BSA), where U=24-h urine creatinine
concentration, V=(total volume of urine collected)/(hours of urine
collection * 60 min), P=serum creatinine and BSA=body surface area (m2).
3. Total protein, alanine aminotransferase (ALT), aspartate
aminotransferase (AST), Hepatitis markers including hepatitis B surface
antigen (HBsAg) and hepatitis C virus (HCV) antibody were measured
Serum ferritin was measured using immulite instrument, based on
two-site chemiluminescent-immunometric assay.[11]
4. Serum and urine bicarbonate were measured by Synchron CX7
auto-analyzer, applying a potentiometric principle.[12]
% FE-HCO3 was
calculated using the standard formula: (urinary bicarbonate / serum
bicarbonate) *100/ (urinary creatinine/ serum creatinine)
5. Serum and urine osmolality were measured by Osmotat030, based on
lowering sample temperature below its freezing point-7°C. Urine/serum
osmolality ratio was then calculated.
6. Colorimetric estimation of total urinary protein was done using
"pyrogallol red" (DiaSys, Diagnostic Systems International, USA), where
proteins-dye form a red complex measured at 600nm.[13]
7. Microalbuminuria was measured by SERA-PAK immuno-microalbumin kit
(Bayer Corporation, Benedict, Eve, Tarry Town, NY, USA).The samples
were mixed with specific antibody, which had polyethylene glycol as an
enhancer and then incubated. Precipitates form a turbidity, which is
directly related to the albumin concentrations, and measured at 340
nm.[14]
8. N-acetyl-BD-glucosaminidase (NAG) was measured by a colorimetric
assay kit. NAG hydrolyzes the substrate
3-cresolsulfonphthaleinyl-N-acetyl-BD-glucosaminidase-sodium salt with
the release of 3-cresolsulfonphtalein sodium salt (3-cresol purple)
which is finally measured photo-metrically at 580nm.[15]
9. Retinol binding protein (RBP) was estimated by applying
enzyme-linked immune-sorbent assay (ELISA) method. The diluted urine
samples were firstly incubated into microplate wells pre-coated with an
antibody specific for RBP. Then the horseradish peroxidase conjugated
antibody was added and further incubated. Following a final washing
step, substrate solution was incubated into the wells resulting in a
colored product and hydrochloric acid, a stopping solution, was added.
The color was measured at 450 nm, and its intensity is proportional to
the amount of RBP present in the sample.[16]
10. Alpha-1 microglobulin assay was estimated by applying an indirect
solid phase enzyme immunoassay kit was used. Calibrators, Controls and
pre-diluted urine samples were firstly incubated into microplate wells
pre-coated with highly purified anti-α1 microglobulin. Then the
horseradish peroxidase conjugate antibody was pipetted into the wells
to form the sandwich complexes. A chromogenic substrate solution was
dispensed and incubated and then hydrochloric acid, a stopping
solution, was added. The optical density was read at 450 nm, and
dichromatic measurement with a 600-690 nm reference reading was
recommended.[17]
Statistical Methods
Statistical analysis was done on a personal computer with SPSS, version 9.05, 1998, USA. The mean, standard deviation and range were calculated. Student t test was performed, for comparative analysis, between groups and Pearson's correlation coefficient (r), was applied for the correlation study. Frequency of renal abnormalities among patients was calculated at cut-off levels corresponding to mean ± 2SD of healthy controls, and X2 test was applied to compare different frequencies. Moreover, Z-score analysis was performed to find out which markers were powerful in identifying patients with renal impairment. Z-score describes the number of SDs, the parameter in a specified group (renal affected patients) away from the negative group (normal renal function patients).
Results
The demographic characteristics and the biochemical parameters of
the patients enrolled were presented in Table 1.
The thalassemic patients demonstrated high level of hepatitis
infection, fifteen patients (16%) had hepatitis infection; eleven of
them were anti-HCV positive, and four were HBsAg positive. Also, the
thalassemic patients showed a significant elevation of the liver
transaminases (ALT, AST), and this was more prominent in splenectomized
β-TM who also showed a significant lower serum albumin and total
protein levels. Fifty percent of β-TI patients were on no iron
chelation therapy compared to only 5% in β-TM patients (p<0.0001).
Deferiprone was the mostly used iron chelator. It was used as a single
chelator by 35% of β-TM patients and 25% of β-TI patients. 20% of β-TM
patients and 15% of β-TI patients were deferoxamine only. 40% of β-TM
patients were on combined deferiprone and deferoxamine chelation
therapy compared to only 10% of β-TI patients. None of our patients was
on the iron chelator deferasirox.
Although serum creatinine and BUN were not statistically different
between thalassemic patients and controls (Table 1), corrected creatinine
clearance were significantly lowered in both groups I and II (P<0.05
and P <0.01, respectively) (Table 2).
Urinary total protein and microalbuminuria were significantly increased
in all thalassemic (β-TM and β-TI) patients (P<0.01).
Urinary tubular markers (NAG, RBP and α-1 microglobulin), were
significantly higher in all thalassemic (β-TM and β-TI) patients
compared to controls. Moreover, β-TM patients showed significantly
higher value in compare to β-TI patients (P<0.01, P<0.05
respectively). Calculated % Fe- HCO3, urine osmolality, and U/S
osmolality were significantly different in all thalassemic patients
versus controls and the effect was more prominent in β-TM patients
(P<0.01) than in β-TI patients (P< 0.05) (Table 2).
Correlation study showed that markers of proximal tubular function
(NAG, RBP and α-1 microglobulin) were negatively correlated with CrCl
(P<0.01, P<0.05, P<0.01 respectively), and were positively
correlated with serum ferritin (P<0.01) and urine total protein
(P<0.01, P<0.05, P<0.01 respectively) (Table 3).
The frequencies of renal abnormalities were calculated in the studied
patients at cut-off levels corresponding to mean±SD of healthy
controls. The most-prevalent renal abnormality was the proteinuria
(71%), followed by increased urinary level of RBP (69.4%), NAG (58.1%),
α-1 microglobulin (54.8%) and microalbuminuria (29%) and also decreased
urinary osmolality (58.1%) (Table 4).
Comparative statistics of the calculated frequencies (Chi-Square test)
revealed that there was a significant difference between the urinary
total protein and both MAU (X2=22.7;
P<0.01) and % FE- HCO3
(X2=18.6; P<0.01) (Table 5)
The Z-score analysis for identifying of patients with renal dysfunction
proved superiority of both urine total protein and RBP as powerful
markers compared to the other studied parameters (Table 6).
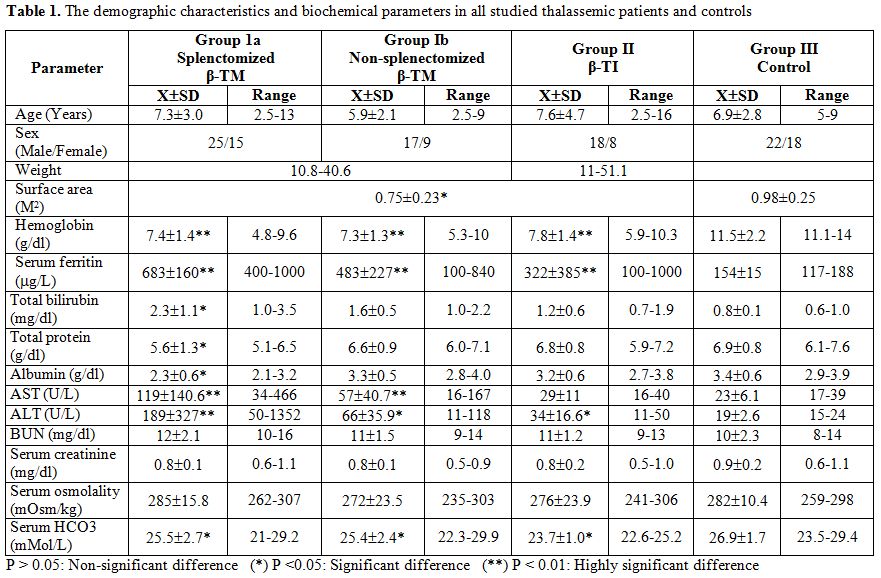 |
Table 1. The demographic characteristics and
biochemical parameters in all studied thalassemic patients and controls
|
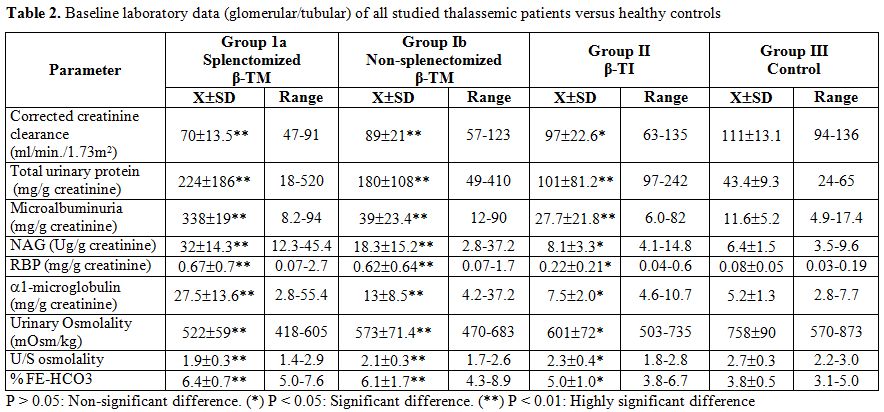 |
Table 2. Baseline laboratory data
(glomerular/tubular) of all studied thalassemic patients versus healthy
controls |
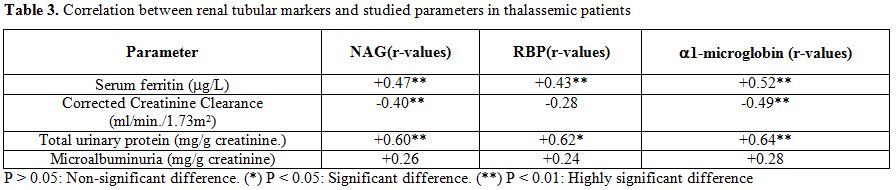 |
Table 3. Correlation between renal
tubular markers and studied parameters in thalassemic patients |
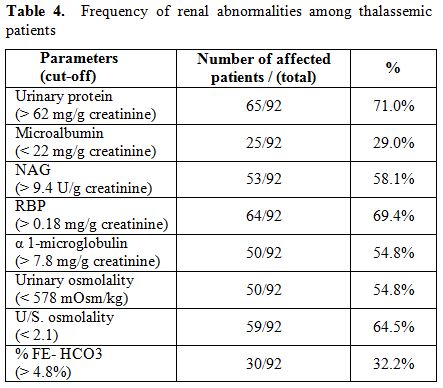 |
Table 4. Frequency of renal abnormalities among
thalassemic patients |
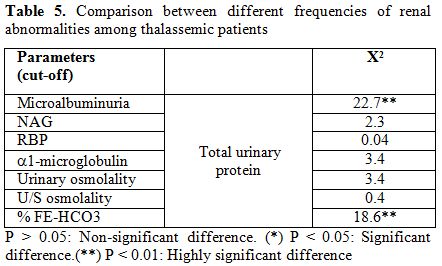 |
Table 5. Comparison between different frequencies
of renal abnormalities among thalassemic patients |
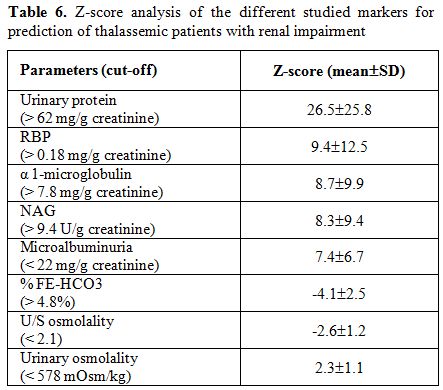 |
Table 6. Z-score analysis of the different
studied markers for prediction of thalassemic patients with renal
impairment |
Discussion
Although advances in the care of patients with β-thalassemia
translate into better survival, this success allowed previously
unrecognized complications to emerge that included several renal
abnormalities.[18] ß-thalassemia major, the severe
form, present in the
first year of life with profound anemia and subsequently require
regular blood transfusions for survival, as well as iron chelation
therapy to treat iron overload and prevent end-organ damage.[19]
ß-thalassemia intermedia present later in life with a milder form of
anemia and remain largely transfusion-independent phenotype.[20] They
develop considerable iron overload due to increased intestinal iron
absorption triggered by the ongoing ineffective erythropoiesis.[21] We
demonstrated elevated levels of serum ferritin in thalassemic patients
reflecting high iron deposition in both β-TM and β-TI, but it was
significantly higher in splenectomized β-TM. Serum ferritin was
positively correlated with the studied markers of tubular function, and
this may provide evidence for the suggested theory of participation of
free iron in proximal tubular dysfunction although the exact mechanism
was not investigated in this work.
Renal tubular dysfunctions have been described previously with
increasing frequency in patients with ß-TM.[22] Many
studies have
demonstrated a proximal tubular damage, leading to increased urinary
excretion of NAG, beta-2 microglobulin, and LMW proteins.[2,23] The
contemporary presence of proteinuria, aminoaciduria, low urine
osmolality[24] and also hyperuricosuria (54%) with
renal uric acid
wasting[25] suggest a more complex damage. Our study
demonstrates a
high frequency of renal abnormalities in the studied children with ß-TM
and ß-TI. The most frequent renal abnormality was proteinuria (71%),
followed by increased urinary level of RBP (69.4%) and NAG
(58.1%), decreased urinary osmolality (58.1%), presence of α-1
microglobulin (54.8%) and microalbumin (29%); these data suggest
complex renal alterations in thalassemic patients, even if in some
patients the tubular dysfunction could be prevalent.
The underlying mechanism for renal dysfunctions in thalassemia patients
is not clear. They seem to be multifactorial, attributed mainly to
include long-standing anemia, chronic hypoxia, iron overload;[24] the
presence of excess unpaired globin chains and high non-hemoglobin iron
content, represent a potential transitional pool of free iron that may
play a major role in lipid peroxidation.[26,27]
Chelation therapy may also affect renal function in thalassaemia
patients. Deferoxamine does not affect the kidneys unless it is given
intravenously, especially at high doses.[28] The new
oral iron
chelator, deferasirox, can cause increases in serum creatinine,
proteinuria, and even renal failure.[29] Awareness of
underlying renal
dysfunction in thalassaemia can inform decisions now about the use and
monitoring of iron chelation.[30] Most of our β-TM
patients were well
chelated, forty percent of them were on combination therapy
deferoxamine and deferiprone and none of the studied patients was
treated with deferasirox, due to its high cost.
In considering the potential mechanisms of renal injury, anemia and
associated potential chronic hypoxia could lead to activation of the
oxidative stress cascade,[31] and may also lead to
changes in the
morphology of cells in terms of size and vascular supply.[32]
A good
correlation between the severity of anemia and markers of tubular
abnormalities are reported in patients with β-TM.[33]
Our patients were
transfused at low hemoglobin level with mean hemoglobin around eight
(g/dl). The scarcity of blood available for the patients justifies this
approach and may reflect the negative cultural attitude towards
blood donation and limited resources of public health system of
developing country like Egypt. This level of anaemia and consequent
hypoxia may explain the high frequency of renal abnormalities in the
studied children with ß-TM and ß-TI.
According the results of this study, abnormalities in GFR are evident
in patients with thalassemia, as demonstrated by occurrence of an
hyperfiltration.[2] Anemia may reduce systemic
vascular resistance, by
determining a hyperdynamic circulation, that increases renal plasma
flow and GFR.[34] That eventually can lead to
stretching of the
glomerular capillary wall and subsequent endothelial and epithelial
injury, which induce transudation of macromolecules into
the mesangium and consequent glomerular dysfunction.[35]
In the
long-term, such changes may lead to a progressive decline in GFR.[36]
In the present work creatinine clearance was the best assessment of
renal total function and was significantly lowered in thalassemic
patients.
The defect of concentrating ability could be caused by increased blood
flow through the vasa recta that could disturb the countercurrent
multiplication effectiveness.[37]
The results of the present work demonstrated a maximal lowering of
urine osmolality in ß-TM patients who had more degree of anemia that is
known to have a hyperperfusion effect. Moreover, the significant
negative correlation of serum ferritin with urine osmolality would
support the previous hypothesis of iron deposition in renal tubules.
Fractional excretion of bicarbonate is a marker of proximal tubular
handling of bicarbonate.4 Preliminary evaluation of bicarbonate
generation of the kidneys revealed a significant elevation of % FE-HCO3
in the thalassemic patients (32.2%) compared to healthy controls.
That suggests a distal tubular defect, whereas a major portion of
patients had elevated LMW proteins as RBP (69.4%) and hyposthenuria
(54.8%). That suggests that distal tubular dysfunction is a late
sequela of the renal tubular involvement in thalassemic patients who
can show an intact handling of bicarbonate.
Examining the pattern of tubular dysfunction among our ß-TM patients
revealed that the degree of defect is more marked in splenectomized
patients than in non-splenectomized group. Indeed, prominent elevation
of NAG and α-1 microglobulin, lowering of urine osmolality and
urine/serum osmolality and also pronounced elevation of serum
ferritin were found more frequently in splenectomized patients.
Ongazyooth and his colleagues also established that tubular defects
were more prominent in splenectomized patients who had higher levels of
serum.[37]
The splenectomized ß-TM patients showed evidences of liver impairment
as manifested by elevated total bilirubin, ALT and lowered total
proteins and albumin. The contribution of viral hepatitis
infection to liver impairment cannot be excluded. Hepatitis B and C,
should be considered also as potential causes of renal disease,[25]
especially when the thalassemic patients demonstrated high level of
hepatitis infection. Fifteen patients (16%) of the present series had
hepatitis infection; eleven of them were anti-HCV antibody positive and
four were HBsAg positive. However, all the positive patients had normal
baseline renal function, and none of them had elevated serum creatinine
above upper normal limit or had a history of nephrotic syndrome,
hypertension or diabetes.
Several researches have demonstrated improved sensitivity and
specificity of measurement of urinary albumin as this is the
predominant urinary protein, for evaluation of glomerular
permeability.[38,39] Our study proved the superiority
of both urinary
total protein and urinary RBP as a powerful marker for identifying
patients with renal dysfunction and so highlighted the importance of
laboratory assay, in the future screening and follow-up programs.
Conclusions
Asymptomatic renal dysfunctions both glomerular and tubular are
prevalent in young β-TM and β-TI patients that then necessitate a
regular screening and follow-up. Urinary total protein and urinary RBP
may be cost-effective markers for early detection of renal dysfunction.
Study Limitations
We did not study uricemia and uricosuria in our thalassemia patients. Further longitudinal prospective studies on a larger number of patients is needed to prove the predictive value of the studied markers.
References
