Occurrence of Secondary Malignancies in Chronic Myeloid Leukemia
During Therapy with Imatinib Mesylate-Single Institution Experience
Grzegorz Helbig1, Grażyna Bober1, Marek Seweryn1, Ryszard Wichary1, Andrzej Tukiendorf2, Lech Sedlak3, Tomasz Oleksy3 and Sławomira Kyrcz-Krzemień1
1 Department of Hematology and Bone Marrow Transplantation, Silesian Medical University, Katowice, Poland.
2 Department of Statistics, Maria Sklodowska-Curie Memorial Cancer Center and Institute of Oncology, Gliwice, Poland.
3
Student Research Group, Department of Hematology and Bone Marrow
Transplantation, Silesian Medical University, Katowice, Poland.
Corresponding author: Grzegorz Helbig, MD, Ph.D.
Department of Hematology and Bone Marrow Transplantation, Silesian
Medical University, Dabrowski street 25, Katowice, Poland. Tel:
+48322591281, fax: +48322554985. E-mail:
ghelbig@o2.pl
Published: January 1, 2015
Received: August 20, 2014
Accepted: November 13, 2014
Meditter J Hematol Infect Dis 2015, 7(1): e2015003, DOI
10.4084/MJHID.2015.003
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Introduction.
Imatinib mesylate (IM) remains the treatment of choice for chronic
myeloid leukemia (CML) showing a remarkable efficacy and offers a
perspective for long disease-free survival. Due to prolonged
administration of IM, the questions about the possible impact on the
development of secondary malignancies (SM) are raised.
Objective. To investigate the incidence and clinical outcome of secondary malignancies during IM therapy for CML.
Material
and Methods. The records of 221 CML patients treated with IM between
2003-2013 in a single institution were reviewed. The Poisson regression
model was used to estimate the relative risks for SM and death in CML
patients.
Results.
Secondary malignancies developed in eight out of the 221 patients
(3.6%) receiving IM for a median of 61 months (range, 10-137 months).
Female/male ratio was 5/3. Two patients were diagnosed with their CML
at accelerated phase whereas 6 had chronic phase. The median age at IM
initiation was 58 years (range, 31-72 years). Five of these 8 SM
patients received IM after other treatments failure: interferon α
(n=5), hydroxyurea (n=4) and cytarabine (n=1). Three patients received
IM as a frontline therapy. All patients were on IM at 400mg daily at SM
occurrence. The therapy for SM included surgery (n=3), chemotherapy
only (n=3), and chemotherapy followed by radiotherapy (n=1). One
patient did not receive treatment due to disseminated disease. All CML
patients were in hematologic and complete cytogenetic response (CCR) at
the time of SM development. All of them also met the criteria for major
molecular response (BCR-ABLIS ≤0.1%).
They continued their IM while receiving treatment for SM. Among eight
patients with SM, five patients are alive and remain in CCR on IM
whereas three patients died due to SM. The risks for SM development as
well as death due to SM in CML patients were not statistically
increased if compared to age-adjusted population.
Conclusions. The association between IM therapy for CML and SM development has not been found.
|
Introduction
Chronic myeloid leukemia (CML) is a clonal stem cell disorder
characterized by the translocation t(9;22)(q34;q11) resulting in
creation of the tyrosine kinase chimeric protein BCR-ABL.[1]
Current therapeutic management of CML patients is based on tyrosine
kinase inhibitors (TKI). Imatinib mesylate (IM) is a small molecule
functioning as a signal transduction inhibitor that specifically
targets a set of tyrosine kinase proteins.[2] This
agent is currently used as a treatment of choice for patients with CML
showing a remarkable efficacy and providing a perspective for a long
disease-free survival.[3] However, due to the
prolonged survival and continuous administration of this agent, the
questions about the possible impact on the development of secondary
malignancies (SM) are raised. IM was found to possess an
immunomodulatory effect on T-cell population as well as dendritic cells
changing the immunologic microenvironment.[4] Data on
the possible pathogenic relationship between the development of SM and
IM administration are inconclusive and require further investigations.[5,6]
Herein,
we investigate the occurrence, and clinical outcome of SM in CML
patients treated with IM. One of those patients with testicular cancer
has been extensively published elsewhere.[7]
Material and Methods
Two hundred and twenty-one CML patients during IM therapy in our
institution between 2003-2013 were included in this analysis. There was
population-based material. All patients followed the common standards
for CML treatment and cytogenetic/molecular monitoring. Shortly, both
cytogenetic and molecular assessments were performed at baseline, then
every three months for the first year and every six months thereafter.
The records of all included patients were reviewed to assess IM doses,
response to therapy and clinical outcome. We divided our CML population
into two age groups: 1/ ≤65 and 2/ >65 years. The “younger”
subgroup included 190 CML patients who developed 7 SM with two deaths
due to SM. The “older” group consisted of 31 CML patients who developed
1 SM with fatal outcome.
Statistical Analysis
The Poisson regression method using WinBUGS software was used to estimate the relative risks for SM and death in CML patients.
Results
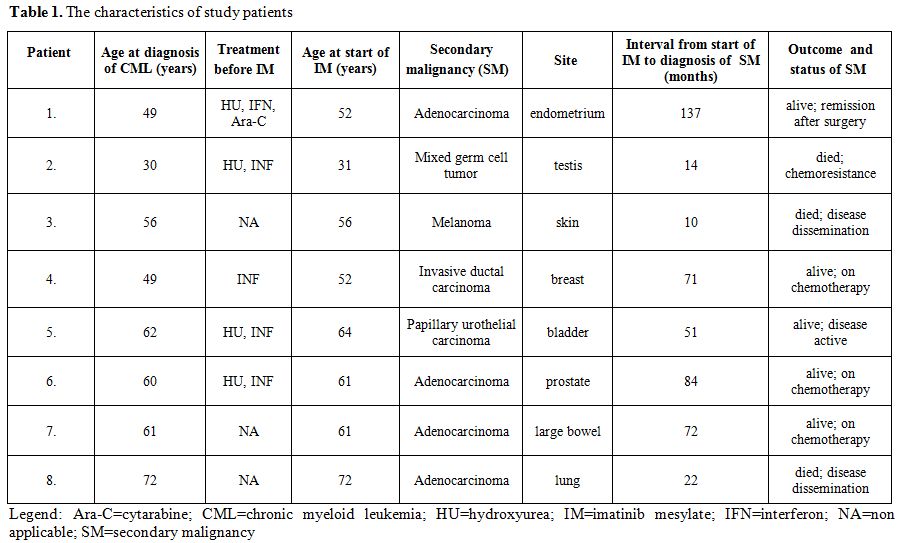
SM were diagnosed in eight out of the 221 patients (3.6%) receiving
IM for a median of 61 months (range, 10-137 months). Female/male ratio
was 5/3. Two patients were diagnosed with their CML at accelerated
phase whereas 6 had chronic phase. The median age at TKI initiation was
58 years (range, 31-72 years). Five of these 8 SM patients received IM
after other treatments failure: interferon α (n=5), hydroxyurea (n=4)
and cytarabine (n=1). Three patients received IM as a frontline
therapy. All patients were on IM at 400mg daily at SM occurrence, and
they had no prior history of cancer. All patients were white and
developed only one additional cancer. There were eight different
malignancies (see table 1).
The
therapy for SM included surgery (n=3); chemotherapy only (n=3); and
chemotherapy followed by radiotherapy (n=1). One patient did not
receive treatment due to disseminated disease. All CML patients were in
hematologic and complete cytogenetic response (CCR) at the time of SM
development. All of them also met the criteria for major molecular
response (BCR-ABLIS ≤0.1%). All
patients continued their IM while receiving treatment for their SM.
Among eight patients with SM, five patients are alive and remain in CCR
on IM whereas 3 patients died due to SM. Following the estimations, no
statistical differences between the risks for CML (in the reference
population) and the SM (in CML patients) as well as between the age
groups (≤65, >65) were established: mean 1.22 [95% CI; 0.14, 4.15],
p=0.44 and mean 0.60 [95% CI; 0.09, 1.47], p=0.07, respectively.
Moreover, no statistical differences between the risks for the SM (in
CML patients) and for death as well as between the age groups (≤65,
>65) were also found: mean 1.82 [95% CI; 0.07, 8.33], p=0.47 and
mean 3.11 [95% CI; 0.10, 17.2], p=0.41, respectively. In sum, the risks
for SM development as well as for death due to SM in CML patients were
not statistically increased if compared to age-adjusted population. The
summary of SM characteristics in CML subpopulation was shown in table 1.
|
|
Table 1. The characteristics of study patients |
Bispecific
T-Cell Engager (BiTE®)
Antibodies
The
efficacy of IM and other TKIs is unquestionable, and early adverse
effects are well-known. In general, these drugs are well-tolerated, and
most of the side effects are manageable.[3] Some
reports focusing on the oncogenic effect of TKIs have been reported,
but the association between the development of SM and TKIs use remains
unclear. A 2-year preclinical study in animal models has showed the
carcinogenic potential of IM. Papilloma of the preputial and clitoral
glands was observed from a dose of 30 mg per kilogram daily that
corresponds to a dose of 400 mg used in human beings. Renal, urinary,
small intestine, stomach, parathyroid and adrenal gland malignancies
were developed at higher IM doses, namely 60 mg/kg/day. Thus, the risk
of benign or malignant tumors was found to be increased in the
above-mentioned rat models.[8] However, the potential pathogenic relationship between the development of secondary tumors and IM has not been proved so far.
There
are inconsistent reports on the incidence of secondary malignancies in
patients with CML treated with TKIs. The first report comes from 2005.
The secondary tumors were detected in 6 out of the 189 CML patients
treated with IM following IFN failure. The authors suggested an
increased incidence of malignant neoplasms among those patients.
Especially, the incidence of prostate cancer was found to be four times
higher than expected in the population.[5] In
contrast, Pilot et al. performed an epidemiological survey of 9518 CML
patients collected in the clinical safety database of Novartis
(imatinib manufacturer). In total, this study showed 110 second primary
neoplasms and the overall incidence of tumors in this subpopulation was
comparable with that of the age-adjusted general population.[6]
Since then, numerous multicenter epidemiological reports have been
published. The Imatinib Long Term Effects study detected 30 cases of SM
in 832 CML patients with an incidence comparable to the expected.
Prostate and breast cancers were the most frequent neoplasms.[3]
Interestingly, a large analysis of 1445 patients with CML and other
hematologic malignancies treated with TKIs suggested a lower than
expected rate of neoplasms in patients treated with TKIs with
observed/expected (O/E) ratio of 0.6. Nevertheless, the incidence of
melanoma, endocrine tumors, kidney cancers, and chronic lymphocytic
leukemia was higher than expected.[9]
On the
other hand, there were several reports demonstrating an increased risk
of secondary neoplasms in CML patients receiving TKIs. The
retrospective analysis of CML population treated with TKIs in Czech
Republic, and Slovakia demonstrated the incidence of secondary
malignancies of 3.3%. The prevalence of all malignant tumors except
non-melanoma skin cancers was 6.7/1000 person-years, and that is 1.5
times higher than the age-adjusted incidence rate. Median time from the
start of TKI therapy to the diagnosis of SM was 32 months.[10]
These data were in line with a report of a German CML study group. A
slight increase of SM in CML patients under TKI treatment if compared
with the general population has been demonstrated. The most common
neoplasms were prostate, colon and lung cancers, as well as non-Hodgkin
lymphomas.[11] Moreover, Japanese authors reported
the incidence of secondary neoplasms after TKI therapy to be 16% at ten
years in a single institution study that is higher than described in
previous reports. It should be mentioned that the tumors developed
after a median time of 24 months after TKI administration.[12]
Recently, Shah et al. have published a population study based on The
Surveillance, Epidemiology, and End Results (SEER) database to evaluate
the incidence of second primary malignancies in CML patients in pre-
and post- imatinib eras. It has been shown that the rate of SM in
post-imatinib era was significantly higher when compared with
pre-imatinib era (O/E ratio 1.48 versus 1.06, respectively). The
highest risk of tumor development was found to be within 1-11 months
after IM initiation, and a digestive tract was involved the most
frequently.[13] At contrary, a large epidemiological
study, based on the Swedish Cancer Registry, found, in imatinib-naïve
CML patients, an increased incidence of second neoplasms for stomach,
skin, urogenital tract cancers as well as for lymphoid leukemias.[14]
In our study, we did not find an increased risk of SM development.
Prior history of sun exposure for melanoma or smoking for bladder
cancer was negative. The impact of pre-imatinib treatments on the SM
occurrence should be excluded as no strong evidence of their
cancerogenic effect does exist. If compared with other studies, the
median time from IM initiation to SM detection was longer and exceeded
five years.[10,13] We did perform
an additional analysis including CML patients treated with second
generation TKI and found no secondary malignancies in this study
subgroup. It may be due to a lower number of patients treated with
second generation TKI if compared with those on imatinib. A shorter
duration of therapy/observation may also be involved.
Based on the
above-mentioned reports one may ask whether there is an association
between IM use and the development of SM. It was demonstrated that this
agent has an immunoregulatory effect by inhibiting T-cell activation
and proliferation as well as by diminishing the capacity of dendritic
cells to elicit primary T-cell responses.[15] The
exposure to IM induces centrosome and chromosome aberrations in
cultures of normal human dermal fibroblasts, Chinese hamster embryonal
and Indian muntjac fibroblasts in a significant, dose-dependent and
species-independent manner. Those aberrant karyotypes emerging under IM
use were irreversible after a prolonged culture omitting the drug.
Thus, these observations suggest that neoplastic, chromosomally
unstable clones may be developed de novo from normal non-hematopoietic
cells by IM.[16] Genetic instability caused by
centrosome defects has an important influence in early steps of the
development as well as in the progression of many cancers.[17,18,19]
Moreover, the c-Abl tyrosine kinase was found to promote DNA
damage-induced apoptosis. The inhibition of apoptosis associated by
TKIs may also explain a proliferative potential of those drugs.[20]
Conclusions
There
is insufficient data to assess that there is an increased risk of
developing SM after IM therapy as well as to elucidate the mechanisms
through the drug can facilitate carcinogenesis. The “over-risk” of SM
occurrence seen in some studies may result from observational bias; CML
patients are simply more carefully monitored than the average
population. One should consider three different scenarios: 1) a
carcinogenic effect of IM therapy, 2) a result of an increased risk of
the development of malignancy with ageing in patients with CML, and
finally 3) a coincidental occurrence of these two neoplasms in this
patient cohort. In sum, it seems reasonable to report all SM that may
develop during or after TKIs treatment. Moreover, further molecular
studies evaluating carcinogenicity of TKIs would be useful.
References
- Sawyers CL. The bcr-abl gene in chronic myelogenous leukaemia. Cancer Surv. 1992; 15:37-51. PMid:1451113

- Buchdunger
E, Zimmermann J, Mett H, Meyer T, Muller M, Regenass U, Lydon NB.
Selective inhibition of the platelet-derived growth factor signal
transduction pathway by a protein-tyrosine kinase inhibitor of the
2-phenylaminopyrimidine class. Proc Natl Acad Sci USA. 1995; 92:
2558-2562. http://dx.doi.org/10.1073/pnas.92.7.2558 PMid:7708684 PMCid:PMC42257
- Gambacorti-Passerini
C, Antolini L, Mahon FX, Guilhot F, Deininger M, Fava C, Nagler A,
Della Casa CM, Morra E, Abruzzese E, D'Emilio A, Stagno F, le Coutre P,
Hurtado-Monroy R, Santini V, Martino B, Pane F, Piccin A, Giraldo P,
Assouline S, Durosinmi MA, Leeksma O, Pogliani EM, Puttini M, Jang E,
Reiffers J,Valsecchi MG, Kim DW. Multicenter independent assessment of
outcomes in chronic myeloid leukemia patients treated with imatinib. J
Natl Cancer Inst. 2011; 103: 553-561. http://dx.doi.org/10.1093/jnci/djr060 PMid:21422402
- Seggewiss
R, Price DA, Purbhoo MA. Immunomodulatory effect of imatinib and second
generation tyrosine kinase inhibitors on T cells and dendritic cells:
an update. Cytotherapy. 2008; 10: 633-641. http://dx.doi.org/10.1080/14653240802317639 PMid:18836918
- Roy
L, Guilhot J, Martineau G, Larchée R, Guilhot F. Unexpected occurrence
of second malignancies in patients treated with interferon followed by
imatinib mesylate for chronic myelogenous leukemia. Leukemia. 2005; 19:
1689-92. http://dx.doi.org/10.1038/sj.leu.2403874 PMid:16015386
- Pilot
PR, Sablinska K, Owen S, Hatfield A. Epidemiological analysis of second
primary malignancies in more than 9500 patients treated with imatinib.
Leukemia. 2006; 20:148. http://dx.doi.org/10.1038/sj.leu.2404025 PMid:16292349
- Kata
D, Mrówka-Kata K, Seweryn M, Pajak J, Najda J, Kyrcz-Krzemien S.
Testicular cancer developed in a chronic myeloid leukemia patient with
a continued complete cytogenetic and molecular response to imatinib. A
case report and review of the literature. Leuk Res. 2010; 34: e229-231.
http://dx.doi.org/10.1016/j.leukres.2010.03.019 PMid:20359744
- Summary of product characteristics of imatinib: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_Product_Information/human/000406/WC500022207.pdf Accessed 10 Feb 2014
- Verma
D, Kantarjian H, Strom SS, Rios MB, Jabbour E, Quintas-Cardama A,
Verstovsek S, Ravandi F, O'Brien S, Cortes J. Malignancies occurring
during therapy with tyrosine kinase inhibitors (TKIs) for chronic
myeloid leukemia (CML) and other hematologic malignancies. Blood. 2011;
118: 4353-4358. http://dx.doi.org/10.1182/blood-2011-06-362889 PMid:21846902 PMCid:PMC3291487
- Voglova
J, Muzik J, Faber E, Zaclova D, Klamova H, Steinerova K, Michalovicova
Z, Demitrovicova L, Cmunt E, Novakova L, Tothova E, Belohlavkova P,
Mayer J, Indrak K. Incidence of second malignancies during treatment of
chronic myeloid leukemia with tyrosine kinase inhibitors in the Czech
Republic and Slovakia. Neoplasma. 2011; 58: 256-262. http://dx.doi.org/10.4149/neo_2011_03_256 PMid:21395367
- Barreto-Miranda
M, Lauseker L, Proetel U, Schreiber A, Hanfstein B, Baerlocher GM, Heim
D, Ehninger G, Hossfeld DK, Kolb HJ, Krause W, Nerl C, Einsele H, Hanel
M, Dengler J, Falge C, Kanz L, Neubauer A, Kneba M, Stegelmann F,
Pfreundschuh M, Waller CF, Spiekermann K, Hofmann WK, Muller MC,
Pfirrman M, Hochhaus A, Hasford J, Hehlmann R, Saussele S. Secondary
malignancies in CML patients - data from the German CML study IV. 2012;
120: Abstract 3746.
- Togasaki-Yoshimoto
E, Shono K, Onoda M, Yokota A. The occurrence of second neoplasms after
treatment with tyrosine kinase inhibitors for chronic myeloid leukemia.
Leuk Lymphoma. 2014; 55: 453-6. http://dx.doi.org/10.3109/10428194.2013.806805 PMid:23697842
- Shah
BK, Ghimire KB. Second Primary Malignancies in Chronic Myeloid
Leukemia. Indian J Hematol Blood Transfus. 2014;
doi:10.1007/s12288-013-0328-2. http://dx.doi.org/10.1007/s12288-013-0328-2
- Rebora
P, Czene K, Antolini L, Passerini CG, Reilly M, Valsecchi MG. Are
chronic myeloid leukemia patients more at risk for second malignancies.
A population-based study. Am J Epidemiol. 2010; 172: 1028-1033. http://dx.doi.org/10.1093/aje/kwq262 PMid:20861143
- Appel
S, Rupf A, Weck MM, Schoor O, Brummendorf TH, Weinschenk T, Grünebach
F, Brossart P. Effects of imatinib on monocyte-derived dendritic cells
are mediated by inhibition of nuclear factor-kappa B and Akt signaling
pathways. Clin Cancer Res. 2005; 11: 1928-1940. http://dx.doi.org/10.1158/1078-0432.CCR-04-1713 PMid:15756019
- Fabarius
A, Giehl M, Frank O, Duesberg P, Hochhaus A, Hehlmann R, Seifarth W.
Induction of centrosome and chromosome aberrations by imatinib in
vitro. Leukemia. 2005; 19: 1573-1578. http://dx.doi.org/10.1038/sj.leu.2403861 PMid:15990860
- Pihan
GA, Purohit A, Wallace J, Malhotra R, Liotta L, Doxsey SJ. Centrosome
defects can account for cellular and genetic changes that characterize
prostate cancer progression. Cancer Res. 2001;
61:2212-2219. PMid:11280789
- Pihan
GA, Wallace J, Zhou Y, Doxsey SJ. Centrosome abnormalities and
chromosome instability occur together in pre-invasive carcinomas.
Cancer Res. 2003; 63: 1398-1404. PMid:12649205
- Mayer
F, Stoop H, Sen S, Bokemeyer C, Oosterhuis JW, Looijenga LHJ.
Aneuploidy of human testicular germ cell tumors is associated with
amplification of centrosomes. Oncogene. 2003; 22:3859-3866. http://dx.doi.org/10.1038/sj.onc.1206469 PMid:12813459
- Yuan
ZM, Huang Y, Ishiko T, Kharbanda S, Weichselbaum R, Kufe D. Regulation
of DNA damage-induced apoptosis by the c-Abl tyrosine kinase. Proc Natl
Acad Sci USA. 1997; 94:1437-1440. http://dx.doi.org/10.1073/pnas.94.4.1437 PMid:9037071 PMCid:PMC19809
[TOP]