The Diagnostic Value of Pulsed Wave Tissue Doppler Imaging in
Asymptomatic Beta- Thalassemia Major Children and Young Adults;
Relation to Chemical Biomarkers of Left Ventricular Function and Iron
Overload
Seham M Ragab1, Waleed M Fathy2, Walaa FAbd El-Aziz3 and Rasha T Helal2
Departments of Pediatrics1, Clinical pathology2 and Cardiology3, Faculty of Medicine, Menoufia University. Naser street, Shebeen El-koom, Menoufia, Egypt.
Corresponding author: Dr Surbhi Goyal MD, DNB. Senior resident,
Department of Pathology, University College of Medical Sciences,
University of Delhi.
Dilshad garden, Delhi-110095. Tel: 91-9873896416. E-mail:
dr.surbhi4you@gmail.com
Published: August 24, 2015
Received: May 17, 2015
Accepted: July 15, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015051, DOI
10.4084/MJHID.2015.051
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Background: Cardiac iron
toxicity is the leading cause of death among β-thalassaemia major (TM)
patients. Once heart failure becomes overt, it is difficult to reverse.
Objectives: To investigate non-overt cardiac dysfunctions in TM
patients using pulsed wave Tissue Doppler Imaging (TD I) and its
relation to iron overload and brain natriuretic peptide (BNP).
Methods: Thorough
clinical, conventional echo and pulsed wave TDI parameters were
compared between asymptomatic 25 β-TM patients and 20 age and gender
matched individuals. Serum ferritin and plasma BNP levels were assayed
by ELISA.
Results: TM patients had significant higher
mitral inflow early diastolic (E) wave and non significant other
conventional echo parameters. In the patient group, pulsed wave TDI
revealed systolic dysfunctions, in the form of significant higher
isovolumetric contraction time (ICT), and lower ejection time (E T),
with diastolic dysfunction in the form of higher isovolumetric
relaxation time (IRT), and lower mitral annulus early diastolic
velocity E` (12.07 ±2.06 vs 15.04±2.65,P=0.003) compared to the
controls. Plasma BNP was higher in patients compared to the controls.
Plasma BNP and serum ferritin had a significant correlation with each
other and with pulsed wave conventional and TDI indices of systolic and
diastolic functions. Patients with E/E` ≥ 8 had significant higher
serum ferritin and plasma BNP levels compared to those with ratio <
8 without a difference in Hb levels.
Conclusion: Pulsed
wave TDI is an important diagnostic tool for latent cardiac dysfunction
in iron-loaded TM patients and is related to iron overload and BNP.
|
Introduction
Thalassemia is one of the most
common genetic disorders. Thus, it is considered a global health
problem. Worldwide, about 5% of the population carry globin variants.
Beta (β)–Thalassemia is caused by the reduced synthesis of β-globin
chains, which leaves an erythrocyte excess of unopposed α-chains
resulting in ineffective erythropoiesis and chronic hemolytic anemia.[1]
According
to the severity, β-thalassemias are classified into: transfusion
dependent β thalassemias (TDT) or β-thalassemia major (TM), non
transfusion dependent β-thalassemia (NTDT) or β- thalassemia intermedia
(TI) and β -thalassemia trait (asymptomatic carriers). β–TM is the
severest form that develops during the first year of life and requires
lifelong transfusion therapy for survival.[2]
Although improving
survival, repeated blood transfusion regimen causes iron overload and
iron toxicity in different organs including the heart.[3]
Despite the progress in iron chelation therapy, congestive heart failure due to iron accumulation
Is still the leading cause of death in β-TM patients.[4,5]
Iron
overload in combination with other inflammatory and immunogenetic
factors can cause left ventricular systolic dysfunction, dilatation and
failure, whereas the sole iron overload may result in left ventricular
diastolic dysfunction with myocardial restriction and subsequent
pulmonary hypertension and right ventricular dilatation.[6]
Patients
with TM may remain asymptomatic and global left ventricular (LV)
function may be preserved until late in the disease process.[7,8] So,
early detection of myocardial dysfunction may be useful in the
management plan.[9]
Echocardiography is an essential imaging
modality for diagnosis of ventricular function,[10] that allows
exclusion of overt LV systolic dysfunction (left ventricular ejection
fraction < 50%).[11]
However, changes of segmental wall motion
– the early sign of myocardial dysfunction in thalassemia patients -
may be subtle and could be missed by conventional echocardiographic
examination which may remain normal until late stages during this
disease process.[12]
Tissue Doppler Imaging (TDI) is a relatively
new Doppler ultrasound modality that records regional systolic and
diastolic velocities within the myocardium. It allows quantitative
measurement of both systolic and diastolic velocities directly from the
ventricular myocardium with the determination of the extent of mitral
annular displacement in systole and diastole.[13]
This new
technique can show additional information compared with other
echocardiography techniques, detecting even minor changes before the
occurrence of abnormal indices of global ventricular dysfunction.[14]
Brain
natriuretic peptide (BNP) is one of the natriuretic peptide system that
is stored in the myocardial cells as pre- proBNP. It is secreted from
the heart as a result of direct wall stress, caused by either stretch
or pressure affecting cardiocytes. Once released, BNP has pronounced
natriuretic, diuretic and vasodilating properties, working to
dramatically reduce volume overload and hypertension.[15] BNP level is
useful for the diagnosis of left ventricular systolic and diastolic
dysfunctions and is correlated with the severity and prognosis.[16,17]
So,
the aim of this work was to investigate the utility of pulsed wave DTI
to detect latent or non-overt cardiac dysfunctions in asymptomatic TM
patients and its relation to the iron overload assayed by serum
ferritin and to BNP as a biomarker of cardiac dysfunction.
Materials and methods
This is a cross-sectional study, performed upon 45 subjects
(patients and controls); 25 β-TM patients and 20 age and sex matched
healthy individuals as controls.
The
patient group included 25
multi-transfused β-TM patients (14 males and 11 females). Their ages
ranged from 4 to 20 years with mean age of 12 ± 5.79 years and median
of
12 years. These patients were kept on a regular blood transfusion
regimen (every 3-4 weeks) since infancy to maintain pre-transfusion Hb
above 7 gm/dl and post-transfusion Hb above 10gm/dl. They were on
long-term chelation therapy for at least one year either by
Deferoxamine (DFO) monotherapy, 30–50 mg/kg body weight by subcutaneous
infusion with an infusion pump for 8–12 h, 5 days per week (16/25=64%),
oral Deferasirox monotherapy, 20-30 mg/kg/day, daily (4/25=16%) or
combined therapy with DFO and Deferasirox (DFO at the dosage of 40
mg/kg/day for 3 days/week and daily Deferasirox at the dosage of 30
mg/Kg/day, 5/25=20%).
The study included cardiac asymptomatic TM
patients with ejection fraction >55% and a normal resting 12-lead
electrocardiogram (ECG).
Patients on cardiovascular treatment,
with any cardiovascular complaints, documented arrhythmia,
hypertension, renal disease, diabetes mellitus, congenital or rheumatic
heart disease, use of medications altering myocardial functions or a
history of smoking were excluded. Also, those who developed transfusion
associated circulatory overload (TACO) or transfusion-related
acute lung injury (TRALI) were excluded.
The control group
consisted of 20 healthy age and gender-matched subjects (10 males and
10 females).Their ages ranged from 4 to 18 years with mean age of 10.9
± 4.86 years and median of 10 years. They were free from acute
(especially viral illness) or chronic illness (including cardiac
diseases) with no family history of chronic hemolytic anemia. All
controls had normal complete blood count (CBC), Hemoglobin (Hb)
electrophoresis with normal ECG and conventional Echocardiographic
findings. They had been randomly selected from children presented to
our general outpatient clinic for routine check up especially for
growth, or for non-specific complaints like non-specific abdominal pain.
This
study had been carried out at the Hematology Unit, Pediatric Department
in collaboration with Clinical Pathology and Cardiology Departments,
Faculty of Medicine, Menoufia University, Egypt, in the period of time
between January 2012 and September 2013.The study was approved by the
ethical committee of Menoufia Medical School, and informed consent was
obtained from the patient or his or her legal guardian.
Methods:
All participants in the study were subjected to a full history taking
and comprehensive clinical examination including a cardiac examination.
For
the patient group, a special emphasis was given to the age of the
disease manifestations, time of the first blood transfusion, frequency
of blood transfusion with calculation of red blood cells transfusion
index (RBCsTI) during the last year, chelation therapy details,
hepatic, renal, histories and history of splenectomy.
For all
included children (patients and controls) weight and height were
measured by the standard methods and plotted against age and sex
specific centiles.
The participants were investigated by the following:
I- Conventional Echocardiography
Echocardiography,
in the form of complete two-dimensional, continuous and pulsed wave
echocardiographic examination, was done using ultrasound machine (vivid
9, General Electric Medical Systems, Horton, Norway), equipped with
5MHz variable frequency harmonic –phased array transducer with
simultaneous ECG monitoring, performed without sedation, during normal
respiration in the left lateral decubitus. Images were recorded in the
standard parasternal long axis, apical four and two chamber views.
Conventional Echo-Doppler Measurements
Routine
M-mode, two-dimensional continuous wave Doppler recordings were
obtained for each subject. The left atrial (LA), aortic (AO) diameters
and left ventricular (LV) internal cavity dimensions including left
ventricular end systolic diameter (LVESD) and left ventricular end
diastolic diameter (LVEDD) were determined. LV ejection fraction (EF)
and LV fractional shortening (FS) were measured using Teichholz’s
M-mode formula.[18]
Transmittal flow patterns were obtained by
pulsed-wave Doppler echocardiography from apical four-chamber view. The
peak of early diastolic flow velocity (E), the peak of late diastolic
flow velocity (A) and the ratio of E/A were measured.
II- Pulsed Wave Tissue Doppler Imaging (TDI) Measurements
The
pulsed wave TDI was performed using the same machine. To display tissue
velocities; from the apical 4 and 2-chamber views, the Doppler sample
volume was placed at four different sites of the mitral annulus:
anterior, lateral, septal and inferior walls in order to record major
velocities. The following parameters were registered: mitral annulus
systolic velocity (S`), mitral annulus early diastolic velocity (E`),
mitral annulus late diastolic velocity (A`) and time intervals;
isovolumetric contraction time (ICT), isovolumetric relaxation time
(IRT) and ejection time (ET).
Then calculation of the mean
E/E`(mitral inflow E wave/ E` mitral annulus velocity) ratio was done.
According to the E/E` ratio, patients were classified into: patients
with E/E`≥ 15 (diastolic dysfunction), patients with E/E`≥ 8 but less
than 15 (suspected diastolic dysfunction) and those with E/E`< 8
(without diastolic dysfunction).[19,20]
All pulsed-wave Doppler
and PW-TDI parameters were measured at the end of expiration, at a
sweep speed of 100 mm/s on three consecutive heart beats and the
average for each was taken.
All data were obtained according to the recommendations of the American Society of Echocardiography.[21]
III- Laboratory investigations including:
1- Complete blood count (CBC): using Beckman 750, Int, U.S.A, Auto-counter after calibration.
2-
Serum ferritin level was measured by Enzyme Linked Immune Sorbent Assay
(ELISA) technique (ELISA, GenWay Biotech, Inc, NP 000137, Swiss) on
Microplate reader (Bio-Rad 680 Hercules, California, USA).The mean
yearly serum ferritin level in the previous year was considered (on the
average of 4 determinations) for patients and at the time of sampling
for the controls.
3- Plasma BNP: Three ml venous blood samples
were drawn by sterile vein-puncture on EDTA tube. Blood samples were
immediately centrifuged for 15 minutes at 3000 rpm; plasma samples were
separated then were stored at –20°C until analysis. Plasma BNP level
was measured by ELISA using kits supplied by Ray Biotech, Inc. GA 30092.
For
the patient group, the echocardiographic examination and the blood
sampling for CBC and BNP assay were performed on the fourth day
following blood transfusion.[22]
Statistical analysis:
The data were processed on an IBM-PC compatible computer using SPSS
version 16 (SPSS Inc., Chicago, IL, USA).Continuous parametric
variables were presented as means± SD while for categorical variables
numbers (%) were used.Chi-square test was used for qualitative
variables. The difference between 2 groups was performed by student’s
t-test for parametric continuous variables and Man Whitney (U) test for
non-parametric variables. Pearson correlation (r): was the test used to
measure the association between two quantitative parametric variables
and Spearman correlation coefficient was applied for non-parametric
data. Receiver Operating Characteristic curve (ROC curve) analysis is a
graph of sensitivity against 1- specificity at different cutoff points.
The optimal cutoff point is that gives the highest sensitivity and
specificity. Two-sided p value of < 0.05 was considered
statistically significant.
Results
For the patient group, their ages at diagnosis ranged from 0.5–1.5
years with a mean of 0.77± 0.24 years. The mean age of first blood
transfusion was 0.69 ± 0.21 years with a range of 0.5–1 year. The mean
duration of transfusion treatment was 10.1 ± 5.11 years, that of the
number of the transfusions /year was 11.2 ±1.22 (median of 11
transfusions/year).
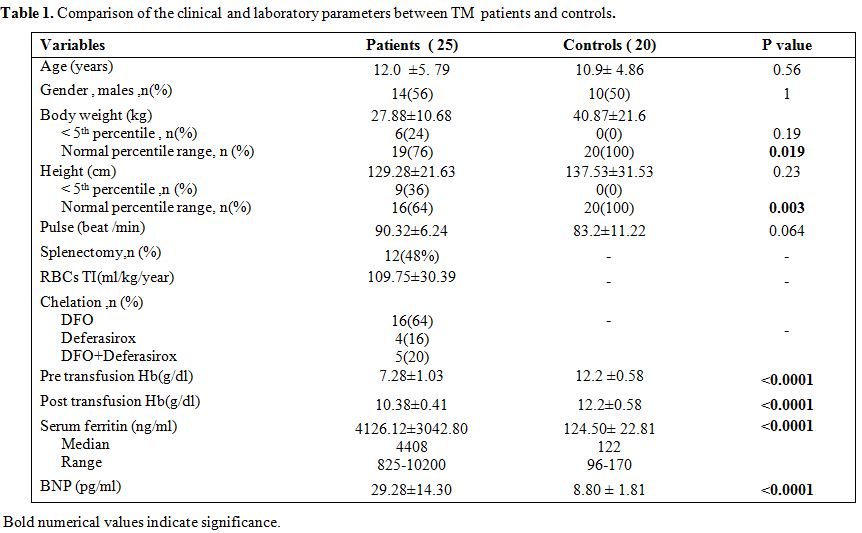
Comparison between the studied groups regarding clinical and laboratory data were represented in Table 1.
The studied groups were matched regarding age, sex, the mean body
weight, the mean height, and pulse rate. History of splenectomy was
documented in 12 (48%) of TM patients. The patient group had a
significantly lower post-transfusion Hb level with significantly higher
mean yearly serum ferritin and plasma BNP levels.
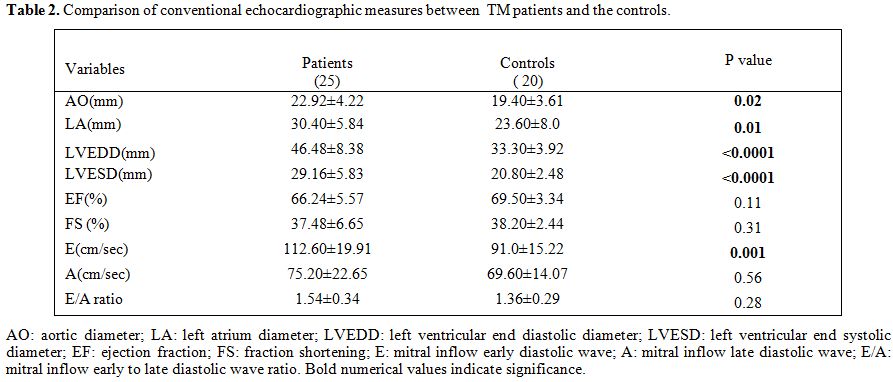
The conventional echocardiography parameters were presented in Table 2.
Compared to the controls, TM patients had significant higher AO, LA,
LVEDD, LVESD diameters and the mitral inflow early diastolic wave
velocity (E). No significant difference was found between the studied
groups regarding the left ventricular EF, left ventricular FS, the
mitral inflow late diastolic wave velocity (A) or the E/A ratio.
|
|
Table 1. Comparison of the clinical and laboratory parameters between TM patients and controls. |
|
|
Table 2. Comparison of conventional echocardiographic measures between TM patients and the controls. |
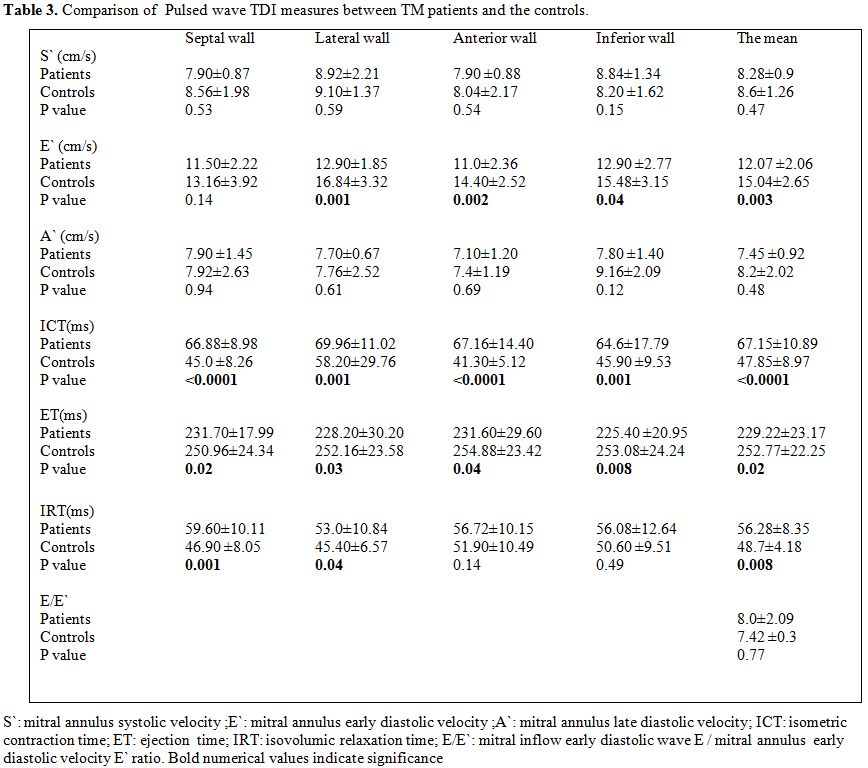
As regard to the pulsed wave TDI parameters (Table 3),
TM patients had significant higher ICT and lower ET compared to the
controls in all tested sites of the mitral annulus as well as in the
mean values of these parameters. The mean IRT and its values at the
septal and the lateral walls of the mitral annulus were significantly
higher in TM compared to the controls. The mean E` as well as its
values at the lateral, anterior and inferior walls of the mitral
annulus were significantly lower in TM patients compared to the
controls. No significant difference was found in the S` or A` between
the studied groups at any of the tested mitral annulus walls or in the
mean values. TM patients had non-significant difference in E/E` ratio
in comparison to the controls. Abnormal E/E` (mitral inflow E wave/E`
mitral annulus velocity) ratio (≥15) was not found in any of TM
patients. According to E/E`, TM patients were classified into those
with E/E` <8 (16 patients, 64% ) and those with this ratio ≥ 8 but
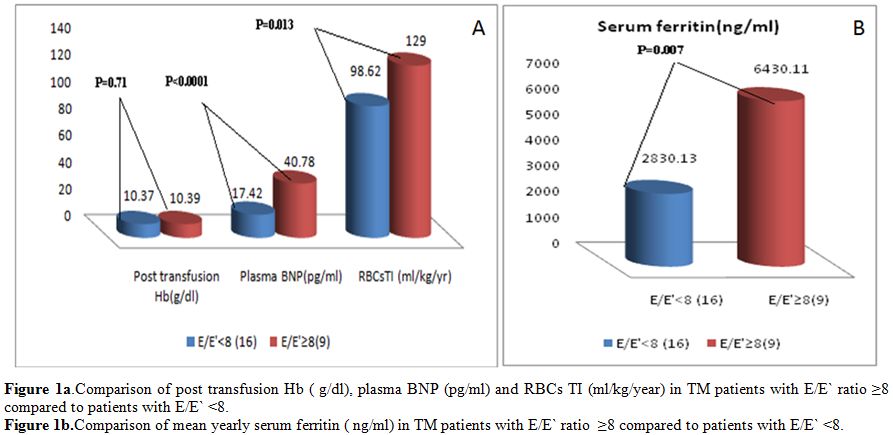
less than 15 (9 patients, 36%). Patients with E/E` ≥ 8 exhibited
significant higher RBCs TI , mean yearly serum ferritin and plasma BNP
levels compared to those with E/E` ratio < 8 without difference in
post-transfusion Hb levels (Figure 1 A and B).
|
|
Table 3. Comparison of Pulsed wave TDI measures between TM patients and the controls. |
|
|
Figure
1A. Comparison of post transfusion Hb ( g/dl), plasma BNP (pg/ml) and
RBCs TI (ml/kg/year) in TM patients with E/E` ratio ≥8 compared to
patients with E/E` <8.
Figure
1B.Comparison of mean yearly serum ferritin ( ng/ml) in TM patients
with E/E` ratio ≥8 compared to patients with E/E` <8. |
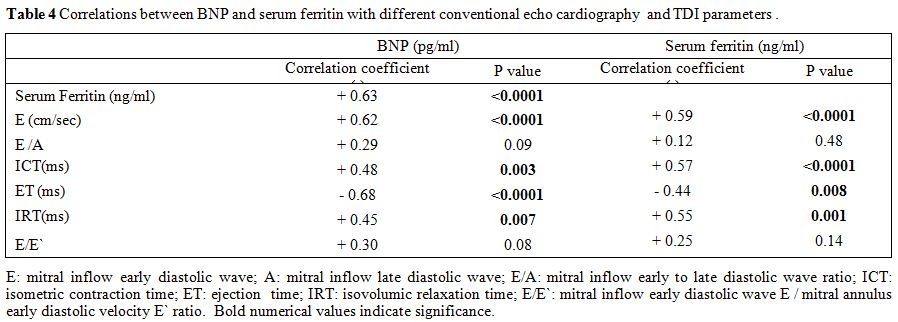
Univariate analysis
among TM patients revealed that serum ferritin and plasma BNP were
positively correlated with each other and each of them had significant
positive correlation with the mean values of E, ICT, and IRT;
significant negative correlation with ET without significant
correlation with E/A or E/E` ratios (Table 4).
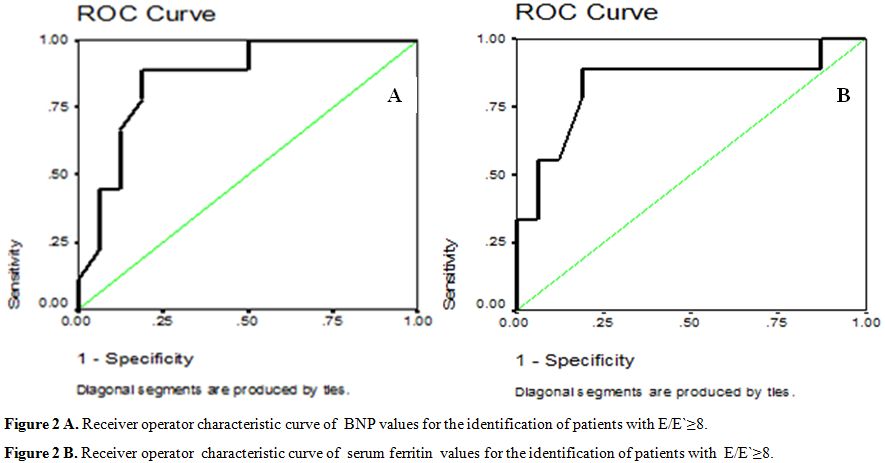
The
data, obtained from the Roc Curve, showed that the best sensitivity of
100% and specificity of 81.9% for the plasma BNP were at cutoff point
of 28.5 pg/ml in ruling out diastolic dysfunction (E/E< 8). Negative
predictive value was 100 % while positive predictive value was 75%.The
area under the curve was 0.86, P = 0.003 (95% CI = 0.71 – 1.01) (Figure 2A).
For
the mean yearly serum ferritin , the data obtained from the Roc Curve
revealed that serum ferritin level at cutoff point of 4790.5 ng /ml had
the best sensitivity of 88.9% and specificity of 81.2% in ruling out
diastolic dysfunction (E/E< 8). Negative predictive value was 92.9%
while positive predictive value was 72, P =0.007. The area under the
curve was 0.83 (95% CI = 0.64 – 1.02) (Figure 2B).
|
|
Table
4. Correlations between BNP and serum ferritin with different conventional echo cardiography and TDI parameters . |
|
|
Figure 2A. Receiver operator characteristic curve of BNP values for the identification of patients with E/E`≥8.
Figure
2B. Receiver operator characteristic curve of serum
ferritin values for the identification of patients with
E/E`≥8.
|
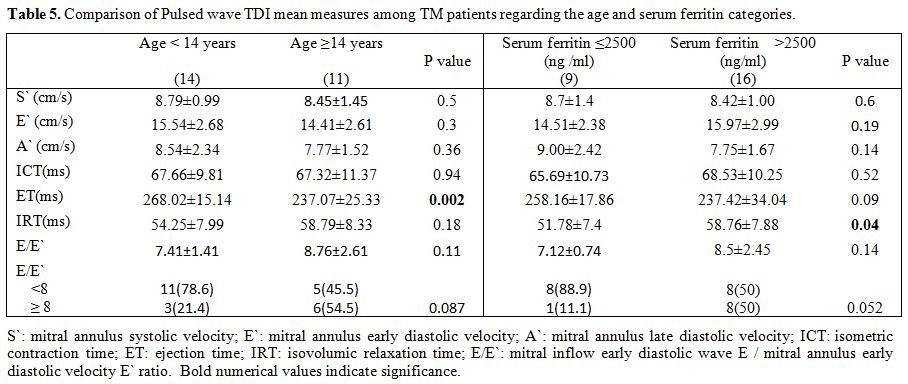
Comparison
of the pulsed wave TDI mean parameters regarding the age and serum
ferritin categories (age of <14 years and ≥ 14years ; serum ferritin
≤2500 ng/ml and > 2500 ng/ml ) revealed that the ET was
significantly lower in TM patients ≥ 14 years compared to those < 14
years. TM patients with serum ferritin >2500 ng/ml had significantly
higher IRT compared to those with serum ferritin level ≤ 2500 ng/ml.
There was no significant difference in the age categories regarding
E/E` ratio < 8 or ≥ 8, while there was a trend of prevalent E/E`
ratio < 8 in those with serum ferritin ≤ 2500 ng/ml (P=0.052) (Table 5).
|
|
Table
5. Comparison of Pulsed wave TDI mean measures among TM patients regarding the age and serum ferritin categories.. |
Discussion
Cardiac
failure due to iron overload remains the most common cause of death in
β-TM patients accounting for up to 71% of all deaths from this disease.[3]Although
intense iron chelation therapy can prevent and delay myocardial
dysfunction, once dysfunction has become clinically evident, it is
difficult to reverse.[23]In
this study, M-mode conventional echocardiography revealed a significant
elevation in LV dimensions (LVEDD and LVESD) in the studied TM patients
compared to the controls, which is concordant with what was reported by
other investigators.[10,24,25] This
cardiac dilatation is attributed to cardiac compensation and adaptation
to the chronic high-output anemic state and hypoxia.[26]In accordance with previous studies,[20,27]
in our study asymptomatic TM patients had a mean values of LVEF and FS
comparable to those of the control group suggesting preserved systolic
function, as assessed by M-mode conventional echocardiography, till
late in the disease. However, other studies reported a significantly
lower LVEF in thalassemia patients in comparison with healthy age and
sex-matched individuals.[28,29]Echocardiographic
evaluation of diastolic functions has been traditionally performed by
measurement of trans-mitral flow parameters including the early (E) and
late (A) diastolic filling velocities and the E/A ratio with
conventional pulsed wave Doppler. The trans-mitral E wave is related to
the time course of active LV relaxation that generates a pressure
gradient from the left atrium through the LV inflow tract.[30]In
this study, mitral E velocity was higher in patients than in controls
without a significant difference in the A velocity or E/A ratio.
Similar results were reported in other studies.[14,24,29,31]
Absence of a significant difference in E/A ratio in TM patients
compared to the controls could be due to the exclusion of patients with
heart failure symptoms. It could be that the E/A alone is not
sufficient to diagnose diastolic dysfunction.[29]Nevertheless, different patterns of abnormality were documented by other researchers,[27,32]
who found a significant reduction in both E and A velocities in TM
patients than controls without significant alteration in E/A ratio.
Moreover, E/A ratio was found to be increased in thalassemia patients
in the study done by Garadah et al.,[33] denoting restrictive diastolic dysfunction. In this regard, out of our studied [25]
TM patients, only 2 were found to have E/A ratio > 2 (denoting
restrictive filling pattern - grade 3 diastolic dysfunction) while the
others had this ratio between 1 and 2 (normal value). It has been
postulated that myocardial iron deposition in some TM patients may not
directly affect left ventricular contractility, but it may rather cause
left ventricular myocardial restriction causing this restrictive
diastolic dysfunction.[34]In
fact, LV diastolic function, as measured by conventional pulsed Doppler
transmitral flow recordings, is limited by its dependence on age and
loading conditions.[22]So,
elevated E velocity among our studied TM patients who were anemic
compared to the controls without higher mean E/A ratio reflects an
increase in the preload state due to chronic anemia.[35]
However, considering the 2 patients with E/A ratio > 2, iron
deposition was the contributing factor that dominated the preload state
resulting in this restrictive pattern.Cardiac iron deposition in TM patients was found to be patchy and more in myocytes rather than the interstitium.[36] This contributes to regional wall motion abnormalities found in these patients.[37]Pulsed
wave TDI can detect regional systolic and diastolic myocardial
dysfunctions earlier than global dysfunction in thalassemia patients.[23] It has the advantage that the measured velocities have been reported to be independent of loading conditions. [38]In
the current study, pulsed wave TDI of TM patients revealed presence of
systolic dysfunction in the form of significantly higher mean and
regional ICT and lower ET values compared to the controls with
non-significant lower regional and mean values of the systolic velocity
S`. TM patients ≥ 14 years old had significant lower mean ET compared
to those below 14 years without any difference in other parameters,
meaning that systolic dysfunction was more evident by increasing age. Significant
reduction in the lateral annulus ejection time of TM patients (age ≤16
years) compared with healthy subjects was reported by Iarussi et al.[14] Furthermore, Abdelmoktader and Azer [28] and Garadah et al.[33] had reported significant lower tissue Doppler systolic velocity in the β-TM group compared to controls. In
terms of diastolic dysfunction indices, the studied TM patients had
significantly lower early diastolic velocity E` and higher IRT.Decreased E` is one of the earliest markers of diastolic dysfunction and is present in all stages of diastolic dysfunction.[13] Reduced E` velocity in TM patients was found by other researchers who attributed this to myocardial stiffness.[28,33]Prolonged IRT had been previously reported in TM patients with normal systolic function.[27,39]
It was suggested that prolonged IRT to be the earliest sign of
diastolic dysfunction in these patients and to reflect iron-induced
impairment in left ventricular relaxation.[39]Combining
trans-mitral flow velocity with annular velocity (E/E`) has been
proposed as a tool for assessing LV filling pressures since it is
influenced by both trans-mitral driving pressure and myocardial
relaxation.[40] Because E` velocity remains reduced
and mitral E velocity increases with higher filling pressure, the ratio
between trans-mitral E and E` (E/E` ratio) correlates well with LV
filling pressure or pulmonary capillary wedge pressure (PCWP).The
subjects have diastolic dysfunction when PCWP is ≥20 mm Hg if E/E` is
≥15, a normal function if E/E` is < 8[19,38] and a suspected diastolic dysfunction having a E/E` ratio between 8 and 15 (grey-intermediate zone).[19,20]The
use of E/E` ratio has provided independent and incremental diagnostic
and prognostic information in some major cardiac diseases, including
heart failure.[13] It has attracted attention for
assessing LV diastolic function due to its load independent nature, its
un-affection by elevated LA pressure and linear correlation with LV end
diastolic pressure.[27]E/E` ratio has a peculiar diagnostic importance for diastolic dysfunction among TM patients.[41]In
this regard, our study results revealed that the mean E/E` of the TM
patients was higher compared to the controls yet the difference did not
reach a significant level (P >0.05). None of the studied TM patients
had E/E`> 15 but in 9 out of the studied 25 patients (36%), E/E`
ratio was in the gray zone, between 8 and 15, while the other 16 (64%)
patients had normal E/E` ratio of <8. Regarding E/E` ratio, both
patient categories had comparable post-transfusion Hb level with higher
serum ferritin and BNP in those with a high ratio. The non-significant
elevation of E/E` ratio is in accordance with Agha et al.[31] but not with Kremastinos et al.[20] and Parale et al.[27]
who found that there was a significant elevation in E/E` in the TM
patients compared to the control group. This difference regarding the
E/E` ratio with the 2 mentioned studies[20,27]
could be related to the difference in the age range, the iron load and
the use of chelation therapy. Actually, our included children were
younger than those of the first study (12.0 ± 5.79 years versus, 27.2 ±
12.5 years for our patients and their patients respectively). Also all
involved patients in our study were under regular chelation therapy
with lower mean yearly serum ferritin level than those of the second
study (4126.12±3042.80 ng/ml versus 8370.85±2660.35 ng/ml respectively)
who did not receive any chelation therapy before. It
is worth mentioning that, our results indicate the absence of global LV
diastolic dysfunction that is in accordance with what was reported
before.[10,22]So,
among our non-symptomatic TM patients having a normal global systolic
function by conventional echocardiography, the pulsed wave TDI had
detected combined latent systolic and diastolic dysfunctions denoting
the importance of this technique. By this, pulsed wave TDI detected
combined systolic and diastolic dysfunctions in thalassemia patients as
in previous reports.[23,28]Considered as a surrogate marker for heart failure,[16,17]
BNP was assayed in this work. Our studied TM patients exhibited
significantly higher BNP compared to the controls being higher in those
with suspected diastolic dysfunction (E/E` ≥ 8). Its level demonstrated
significant correlations with systolic (positive correlation with ICT
and negative correlation with ET) and diastolic (positive correlation
with both E wave and IRT) dysfunction indices, with a positive
correlation trend with E/E` ratio (P= 0.08). BNP also had good
correlation with serum ferritin as an indicator of iron overload.
Elevated BNP in TM patients and its association with diastolic
dysfunction was documented in previous studies.[20,41]Nikolidakis et al.[42]
found that BNP levels were statistically higher in the severely
iron-loaded thalassemia group (with MRI T2* < 24 ms). BNP levels
inversely correlated with myocardial T2 relaxation time values. The
authors adopted a cut-off value of 29 pg/ml (sensitivity of 88%,
specificity of 58%, negative predictive value of 94% and positive
predictive value of 37%) for the identification of patients with severe
myocardial hemosiderosis using magnetic resonance imaging as the
comparative “gold” standard.In
accordance, our results revealed a BNP level of 28.5 pg/ml in ruling
out diastolic dysfunction (E/E`< 8) and to discriminate patients
with E/E` ≥ 8 (suspected diastolic dysfunction) indicating the
importance of BNP in prediction of cardiac iron load and its induced
diastolic dysfunction before conventional indices of systolic function
are affected. Iron overload is the main determinant of cardiac morbidity in TM patients.[4,5]
Although not completely reliable, serum ferritin is the wildly accepted parameter of iron overload in clinical practice.[43]
Single ferritin measurement may be misleading and it does not reflect
long-term ferritin levels or correlate with cardiac iron levels.[44]
However, the yearly trends in ferritin levels may reflect the direction
of body iron loading and long term elevations in ferritin predict
cardiac mortality.[45] By this, the mean yearly serum
ferritin during the last year of our enrolled TM patients, had a
significant relation to pulsed wave conventional and TDI systolic and
diastolic dysfunction indices. It also had significant positive
correlation with BNP, the chemical marker of cardiac dysfunction. In
addition it was significantly higher among patients with E/E` ratio ≥8
than those with this ratio of <8, finding that was coupled with
significant higher RBC s consumption in these patients. However, in
some previous studies, no relation was found between diastolic
dysfunction and serum ferritin level.[28,33]Serum ferritin level of > 2500 ng/ml had been suggested to indicate increased risk of cardiac affection.[3]
The studied TM patients with serum ferritin > 2500 ng/ml had
significantly higher IRT compared to those with serum ferritin level ≤
2500 ng/ml with a trend of prevalent E/E` ratio < 8 (normal
diastolic function) in those with serum ferritin < 2500 ng/ml (P
=0.052). However, using the ROC curve, serum ferritin level of 4790.5
ng/ml was the cutoff value to predict E/E` ratio ≥ 8. In this regards,
El Beshlawy et al.[46] had reported that there
was a low prevalence of myocardial siderosis as measured by
cardiovascular magnetic resonance (MRI T2*) in the Egyptian TM patients
in spite of very high serum ferritin and high liver iron concentration
(LIC). The authors postulated that, the possibility of a genetic
component for the resistance to cardiac iron loading in this population
should be considered. This could reflect genetic susceptibility to
cardiac iron toxicity in different populations and needs further
large-scale studies.In
summary, cardiac dysfunction is a common morbidity among iron-loaded TM
patients despite regular chelation therapy. In this study cardiac
non-symptomatic TM patients with normal global systolic functions by
conventional Echo-Doppler measurements demonstrated abnormal left
ventricular systolic and diastolic indices using the pulsed-wave TDI
study which were correlated with plasma BNP and serum ferritin. This
confirms the importance of this diagnostic modality in TM patients
especially in developing countries where wide use of cardiovascular
magnetic resonance (MRI T2*) is limited by its expensiveness.[23]
BNP cut-off value for prediction of diastolic dysfunction (E/E`≥8) was
more or less equal to the previously documented one for prediction of
MRI T2* < 24 ms (28.5 pg/ml vs 29 pg/ml) and this raise the concern
about the importance of this simple un-expensive test in iron-loaded TM
patients. Conclusions
Asymptomatic TM children under regular chelation therapy may have
latent diastolic and or systolic dysfunctions that could not be
detected by conventional echocardiography but could be highlighted by
TDI. Hence, application of pulsed-wave TDI in these patients is
appropriate. Integrated use of echocardiography, pulsed-wave TDI and
BNP level for an accurate assessment of cardiac functions is highly
recommended to help identifying subjects at risk and facilitates early
intervention
References
- Rund D, Rachmilewitz E. Beta-thalassemia. N Engl J Med. 2005;353: 1135–1146. http://dx.doi.org/10.1056/NEJMra050436 PMid:16162884

- TheinSL. Genetic modifiers of ß-thalassemia. Haematologica . 2005 May; 90(5):651-660 .
- Olivieri
NF, Nathan DG, MacMillan JH, Wayne AS, Liu PP, McGee A, Martin M, Koren
G, Cohen AR.Survival in medically treated patients with homozygous
beta-Thalassemia. N Engl J Med. 1994 Sep 1;331(9):574-578. http://dx.doi.org/10.1056/NEJM199409013310903 PMid:8047081
- Walker JM. The heart in thalassaemia. Eur Heart J.2002 23:102–105. http://dx.doi.org/10.1053/euhj.2001.2850 PMid:11785990
- Borgna-Pignatti
C, Cappellini MD, De Stefano P, Del Vecchio GC, Forni GL, Gamberini MR,
Ghilardi R, Piga A, Romeo MA, Zhao H, Cnaan A. Cardiac morbidity and
mortality in deferoxamine or deferiprone-treated patients with
thalassemia major. Blood. 2006 May 1;107(9):3733-3737. http://dx.doi.org/10.1182/blood-2005-07-2933 PMid:16373663
- Kremastinos
DT, Farmakis D, Aessopos A, Hahalis G, Hamodraka E, Tsiapras D, Keren
A. Beta-thalassemia cardiomyopathy: history, present considerations,
and future perspectives. Circ Heart Fail. 2010 May;3(3):451-458. http://dx.doi.org/10.1161/CIRCHEARTFAILURE.109.913863 PMid:20484195
- Pennell DJ . T2* magnetic resonance and myocardial iron in thalassemia. Ann N Y Acad Sci. 2005;1054:373-378. http://dx.doi.org/10.1196/annals.1345.045 PMid:16339685
- Cohen AR, Galanello R, Pennell DJ, Cunningham MJ, Vichinsky E. Thalassemia. Hematology Am Soc Hematol Educ Program 2004:14-34.
- Hahalis
G, Manolis AS, Gerasimidou I, Alexopoulos D, Sitafidis G, Kourakli A.
Right ventricular diastolic function in beta-thalassemia major:
Echocardiographic and clinical correlates. Am Heart J.
2001;141:428–434. http://dx.doi.org/10.1067/mhj.2001.113077 PMid:11231441
- Hamdy
AM. Use of strain and tissue velocity imaging for early detection of
regional myocardial dysfunction in patients with beta thalassemia. Eur
J Echocardiogr. 2007 Mar;8(2):102-109. http://dx.doi.org/10.1016/j.euje.2006.02.004 PMid:16564231
- Mottram
PM, Marwick TH. Assessment of diastolic function: what the general
cardiologist needs to know. Heart. 2005 May;91(5):681-695. http://dx.doi.org/10.1136/hrt.2003.029413 PMid:15831663 PMCid:PMC1768877
- Leonardi
B, Margossian R, Colan SD, Powell AJ. Relationship of magnetic
resonance imaging estimation of myocardial iron to left ventricular
systolic and diastolic function in thalassemia. JACC Cardiovasc
Imaging. 2008 Sep;1(5):572-578. http://dx.doi.org/10.1016/j.jcmg.2008.04.005 PMid:19356483
- Yu
CM, Sanderson JE, Marwick TH, Oh JK. Tissue Doppler imaging a new
prognosticator for cardiovascular diseases. J Am Coll Cardiol. 2007 May
15;49(19):1903-1914.
http://dx.doi.org/10.1016/j.jacc.2007.01.078 PMid:17498573 - Iarussi
D, Di Salvo G, Pergola V, Coppolino P, Tedesco MA, Ratti G, Esposito L,
Calabrò R, Ferrara M. Pulsed doppler tissue imaging and myocardial
function in thalassemia major. Heart Vessels. 2003 Mar;18(1):1-6. http://dx.doi.org/10.1007/s003800300000 PMid:12644874
- Daniels LB, Maisel AS.Natriuretic Peptides. J Am Coll Cardiol. 2007 Dec 18;50(25):2357-2368. http://dx.doi.org/10.1016/j.jacc.2007.09.021 PMid:18154959
- Sagnella
GA. Measurement and importance of plasma brainnatriuretic peptide and
related peptides. Ann Clin Biochem. 2001 Mar;38(Pt 2):83-93. http://dx.doi.org/10.1258/0004563011900317 PMid:11269760
- Kremastinos
DT, Tsiapras DP, Kostopoulou AG, Hamodraka ES, Chaidaroglou AS, Kapsali
ED. NT-proBNP levels and diastolic dysfunction in ß-thalassaemia major
patients. Eur J Heart Fail. 2007 May;9(5):531-536. http://dx.doi.org/10.1016/j.ejheart.2006.11.004 PMid:17317307
- Teichholz
LE, Kreulen T, Herman MV, Gorlin R. Problems in echocardiographic
volume determinations: Echocardiographic –angiographic correlations in
the presence or absence of asynergy. Am J Cardiol. 1976 Jan;37(1):7-11.
http://dx.doi.org/10.1016/0002-9149(76)90491-4
- Ommen
SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, Tajik AJ.
Clinical utility of Doppler echocardiography and Tissue Doppler imaging
in theestimation of left ventricular filling pressures: a comparative
simultaneous Doppler-catheterization study. Circulation. 2000 Oct
10;102(15):1788-1794. http://dx.doi.org/10.1161/01.CIR.102.15.1788 PMid:11023933
- Kremastinos
DT, Hamodraka E, Parissis J, Tsiapras D, Dima K, Maisel A. Predictive
value of B- type natriuretic peptides in detecting latent left
ventricular diastolic dysfunction in beta-thalassemia major. Am Heart
J. 2010 Jan;159(1):68-74. http://dx.doi.org/10.1016/j.ahj.2009.10.025 PMid:20102869
- Pellikka
PA, Nagueh SF, Elhendy AA, Kuehl CA, Sawada SG; American Society of
Echocardiography. American Society of Echocardiography recommendations
for performance, interpretation, and application of stress
echocardiography. J Am Soc Echocardiogr. 2007;20:1021–1041. http://dx.doi.org/10.1016/j.echo.2007.07.003 PMid:17765820
- Kremastinos
DT, Tsiapras DP, Tsetsos GA, Rentoukas EI, Vretou HP, Toutouzas PK.
Left ventricular diastolic Doppler characteristics in beta-thalassemia
major. Circulation. 1993 Sep;88(3):1127-1135. http://dx.doi.org/10.1161/01.CIR.88.3.1127 PMid:8353874
- Vogel
M, Anderson LJ, Holden S, Deanfield JE, Pennell DJ, Walker JM. Tissue
doppler echocardiography in patients with beta thalassemia detects
early myocardial dysfunction related to myocardial iron overload. Eur
Heart J. 2003 Jan;24(1):113-119. http://dx.doi.org/10.1016/S0195-668X(02)00381-0
- Aypar
E1, Alehan D, Hazirolan T, Gümrük F.The efficacy of tissue Doppler
imaging in predicting myocardial iron load in patients with
beta-thalassemia major: correlation with T2* cardiovascular magnetic
resonance. Int J Cardiovasc Imaging. 2010 Apr;26(4):413-429. http://dx.doi.org/10.1007/s10554-010-9591-6 PMid:20127175
- Uçar
T, Ileri T, Atalay S, Uysal Z, Tutar E, Ertem M.Early detection of
myocardial dysfunction in children with beta-thalassaemia major. Int J
Cardiovasc Imaging. 2009 Apr;25(4):379-386. http://dx.doi.org/10.1007/s10554-008-9404-3 PMid:19107572
- Ehlers
KH, Levin AR, Markenson AL, Marcus JR, Klein AA, Hilgartner MW, Engle
MA . Longitudinal study of cardiac function in thalassemia major. Ann N
Y Acad Sci. 1980;344:397-404. http://dx.doi.org/10.1111/j.1749-6632.1980.tb33678.x PMid:6930879
- Parale
GP, Pawar SS, Tapare VS. Assessment of LV diastolic function in
patients with beta-thalassemia major with special reference to E/E ann
ratio. J Pediatr Hematol Oncol. 2009 Jan;31(1):69-73. http://dx.doi.org/10.1097/MPH.0b013e31818ab138 PMid:19125094
- Abdelmoktader
AM, Azer HY. Usefulness of pulsed wave tissue doppler imaging in
assessment of left ventricular functions in children with
beta-thalassemia major. Indian J Pediatr. 2013 Sep;80(9):721-725. http://dx.doi.org/10.1007/s12098-013-1020-0 PMid:23604609
- Noori
NM, Mehralizadeh S. Echocardiographic evaluation of systolic and
diastolic heart function in patients suffering from beta-thalassemia
major aged 5-10 years at the Zahedan Research Center for Children and
Adolescent Health. Anatolian journal of cardiology. 2010
Apr;10(2):150-153 .
- Nishimura
RA, Tajik AJ. Evaluation of diastolic filling of left ventricle in
health and disease: Doppler echocardiography is the clinician's Rosetta
Stone. J Am Coll Cardiol. 1997 Jul;30(1):8-18. http://dx.doi.org/10.1016/S0735-1097(97)00144-7
- Agha
HM, Beshlawy A, Hamdy M, Sobeih A, El Zahrae F, Abd El Satar IA,
AbdelMassih A, Said F, Abd El Aziz O, El Tagui M, Pennell DJ. Early
detection of right ventricular diastolic dysfunction by pulsed tissue
Doppler echocardiography in iron loaded beta thalassemia patients.
Pediatr Cardiol. 2015 Mar;36(3):468-474. http://dx.doi.org/10.1007/s00246-014-1035-y PMid:25293426
- Seliem
MA, Al-Saad HI, Bou-Holaigah IH, Khan MN, Palileo MR. Left ventricular
diastolic dysfunction in congenital chronic anaemias during childhood
as determined by comprehensive echocardiographic imaging including
acoustic quantification. Eur J Echocardiogr. 2002 Jun;3(2):103-110. http://dx.doi.org/10.1053/euje.2001.0122 PMid:12114094
- Garadah
T, Kassab S, Mahdi N, Abu-Taleb A and Jamsheer A. Pulsed and Tissue
Doppler Echocardiographic Changes in Patients with Thalassemia Major
Clinical Medicine Insights: Cardiology 2010;3 :1–8.
- Kremastinos DT. Heart failure in beta-thalassemia. Congest Heart Fail. 2001;7:312–314. http://dx.doi.org/10.1111/j.1527-5299.2001.00259.x PMid:11828176
- Vaccari
M, Crepaz R, Fortini M, Gamberini MR, Scarcia S, Pitscheider W, Bosi G.
Left ventricular remodeling, systolic function, and diastolic function
in young adults with beta thalassemia intermedia. Chest. 2002
Feb;121(2):506-512. http://dx.doi.org/10.1378/chest.121.2.506 PMid:11834665
- Fitchett
DH, Coltart DJ, Littler WA, Leyland MJ, Trueman T, Gozzard DI, Peters
TJ. Cardiac involvement in secondary haemochromatosis: a catheter
biopsy study and analysis of myocardium. Cardiovasc Res. 1980
Dec;14(12):719-724. http://dx.doi.org/10.1093/cvr/14.12.719 PMid:7260965
- Lattanzi
F, Bellotti P, Picano E, Chiarella F, Mazzarisi A, Melevendi C, Forni
G, Landini L, Distante A, Vecchio C. Quantitative ultrasonic analysis
of myocardium in patients with thalassemia major and iron overload.
Circulation. 1993 Mar;87(3):748-754. http://dx.doi.org/10.1161/01.CIR.87.3.748 PMid:8443895
- Sohn
DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, Lee MM, Park YB, Choi YS,
Seo JD, Lee YW. Assessment of mitral annulus velocity by Doppler tissue
imaging in evaluation of left ventricular diastolic function. J Am Coll
Cardiol. 1997 Aug;30(2):474-480. http://dx.doi.org/10.1016/S0735-1097(97)88335-0
- Gharzuddine
WS1, Kazma HK, Nuwayhid IA, Bitar FF, Koussa SF, Moukarbel GV, Taher
AT. Doppler characterization of left ventricular diastolic function in
beta-thalassaemia major. Evidence for an early stage of impaired
relaxation. Eur J Echocardiogr. 2002 Mar;3(1):47-51. http://dx.doi.org/10.1053/euje.2001.0114 PMid:12067534
- Nagueh
SF, Lakkis NM, Middleton KJ, Spencer WH 3rd, Zoghbi WA, Qui-ones MA.
Doppler estimation of left ventricular filling pressures in patients
with hypertrophic cardiomyopathy. Circulation. 1999 Jan
19;99(2):254-261. http://dx.doi.org/10.1161/01.CIR.99.2.254 PMid:9892592
- Chrysohoou
C, Greenberg M, Pitsavos C, Panagiotakos DB, Ladis V, Barbetseas J,
Brili S, Singh S, Stefanadis C. Diastolic function in young patients
with beta- thalassemia major: an echocardiographic study.
Echocardiography. 2006 Jan;23(1):38-44. http://dx.doi.org/10.1111/j.1540-8175.2006.00148.x PMid:16412181
- Nikolidakis
S, Flessa C, Nikolaou N, Gotsis ED, Koutouzis M, Polyhronaki E, Vrettou
E, Kyriakides ZS. Brain natriuretic peptide as marker of myocardial
iron load in beta-thalassemia.Int J Cardiol. 2007 Jun
12;118(3):408-409. http://dx.doi.org/10.1016/j.ijcard.2006.07.052 PMid:17045671
- Lo L, Singer ST . Thalassemia; current approach to an old disease . Pediatr Clin North Am. 2002 Dec;49(6):1165-91, v. http://dx.doi.org/10.1016/S0031-3955(02)00088-3
- Anderson
LJ1, Holden S, Davis B, Prescott E, Charrier CC, Bunce NH, Firmin DN,
Wonke B, Porter J, Walker JM, Pennell DJ. Cardiovascular T2 star (T2*)
magnetic resonance for the early diagnosis of myocardial iron overload.
Eur Heart J. 2001 Dec;22(23):2171-2179. http://dx.doi.org/10.1053/euhj.2001.2822 PMid:11913479
- Pennell
DJ, Udelson JE, Arai AE, Bozkurt B, Cohen AR, Galanello R, Hoffman TM,
Kiernan MS, Lerakis S, Piga A, Porter JB, Walker JM, Wood J; American
Heart Association Committee on Heart Failure and Transplantation of the
Council on Clinical Cardiology and Council on Cardiovascular Radiology
and Imaging. Cardiovascular function and treatment in b-Thalassemia
major: a consensus statement from the american heart association.
Circulation. 2013 Jul 16;128(3):281-308. http://dx.doi.org/10.1161/CIR.0b013e31829b2be6 PMid:23775258
- El
Beshlawy A, El Tagui M, Hamdy M, El Ghamrawy M, Azim KA, Salem D, Said
F, Samir A, St Pierre T, Pennell DJ. Low prevalence of cardiac
siderosis in heavily iron loaded Egyptian thalassemia major patients.
Ann Hematol. 2014 Mar;93(3):375-379. http://dx.doi.org/10.1007/s00277-013-1876-0 PMid:23949317
[TOP]