Received: April 12, 2017
Accepted: May 22, 2017
Mediterr J Hematol Infect Dis 2017, 9(1): e2017044 DOI 10.4084/MJHID.2017.044
This article is available on PDF format at:

Department of Pathology, Botucatu School of Medicine, São Paulo State University. Brazil.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
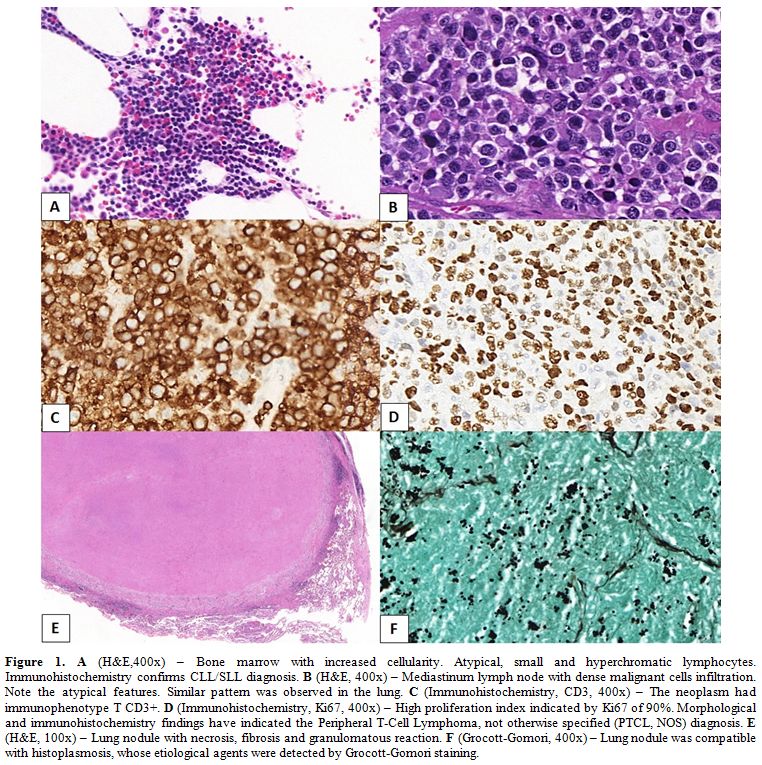 |
Figure 1. A (H&E,400x) – Bone marrow with increased cellularity. Atypical, small and hyperchromatic lymphocytes. Immunohistochemistry confirms CLL/SLL diagnosis. B (H&E, 400x) – Mediastinum lymph node with dense malignant cells infiltration. Note the atypical features. Similar pattern was observed in the lung. C (Immunohistochemistry, CD3, 400x) – The neoplasm had immunophenotype T CD3+. D (Immunohistochemistry, Ki67, 400x) – High proliferation index indicated by Ki67 of 90%. Morphological and immunohistochemistry findings have indicated the Peripheral T-Cell Lymphoma, not otherwise specified (PTCL, NOS) diagnosis. E (H&E, 100x) – Lung nodule with necrosis, fibrosis and granulomatous reaction. F (Grocott-Gomori, 400x) – Lung nodule was compatible with histoplasmosis, whose etiological agents were detected by Grocott-Gomori staining. |
References

[TOP]