We retrospectively analyzed data from 326 MDS, MDS/MPN, and low blast count AML (LBC-AML) patients enrolled to Hellenic MDS registry from July 2004 to May 2017. The data cutoff date for the analysis was July 7, 2017, and the current analysis included only patients who received AZA as 1st line treatment. All patients were treated in a non-clinical trial setting at an initial dose of 75mg/m2 SC for seven days on 28-day cycles. Granulocyte colony-stimulating factors and erythropoiesis-stimulating agents were used at the discretion of the treating physician. Dose reductions of 25%-50% and/or treatment delays were considered for severe myelotoxicity or myelosuppression-related complications. Treatment response was evaluated using the IWG 2006 criteria.[6] Survival analysis was performed using a Kaplan-Meier estimate and Cox’s proportional hazards model. Overall survival (OS) was defined as the time from AZA initiation or failure to last follow up or death from any cause. Akaike Information Criteria with correction for finite sample sizes (AICc) was used to compare model fits.[7]
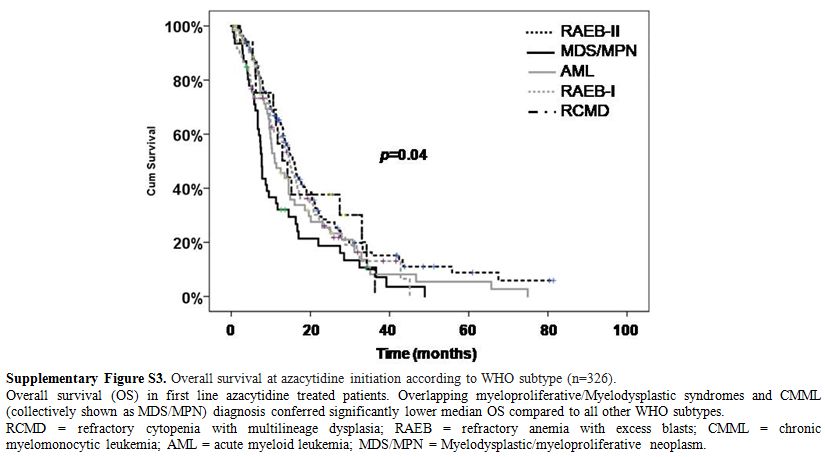
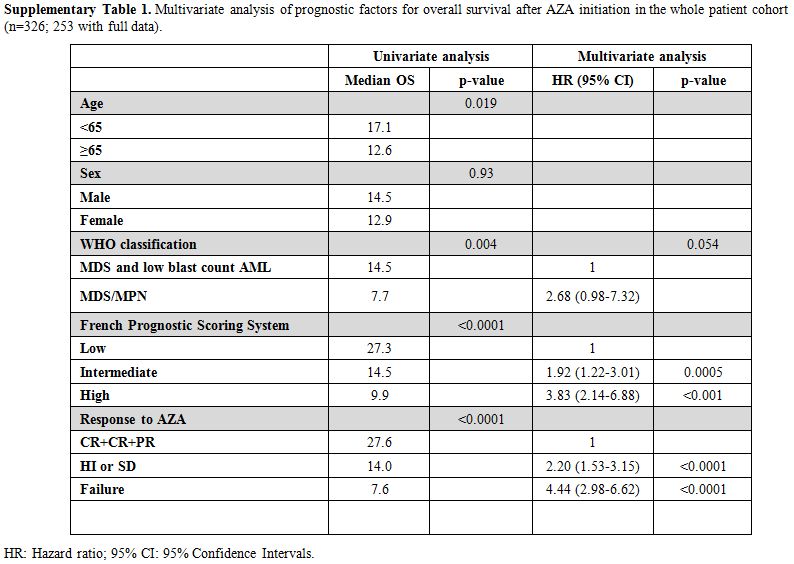
Table 1 lists the patients’ characteristics. After a median follow-up of 41.7 months, the median OS from AZA initiation for the whole cohort was 14 (95% CI: 12.6–15.4) months. Though not designed for patients with MDS/MPN and low-risk IPSS the French Prognostic Scoring System (FPSS)[8] was the better survival discriminator compared to IPSS and IPSS-R (Figure 1A, AICc 1958,841 vs. 2276,767 vs. 2321,742, respectively). In multivariate analysis, FPSS (p<0.001), the best response to AZA (p<0.001) and, marginally, disease subtype (MDS/MPN vs others, p=0.01) were all independent predictors of OS (supplementary Table 1).
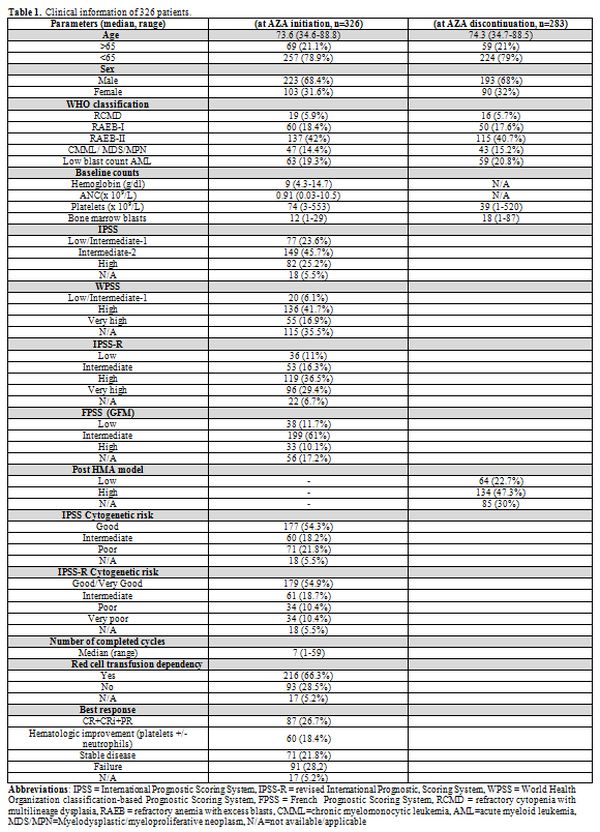 |
Table1. Clinical information of 326 patients. |
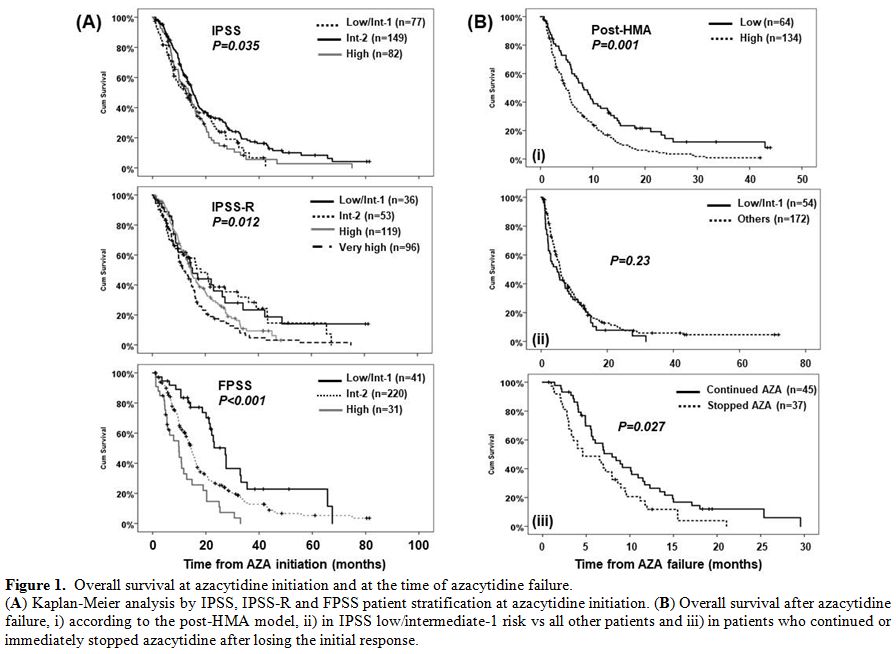 |
Figure 1. Overall survival at azacytidine initiation and at the time of azacytidine failure. (A) Kaplan-Meier analysis by IPSS, IPSS-R and FPSS patient stratification at azacytidine initiation. (B) Overall survival after azacytidine failure, i) according to the post-HMA model, ii) in IPSS low/intermediate-1 risk vs all other patients and iii) in patients who continued or immediately stopped azacytidine after losing the initial response. |
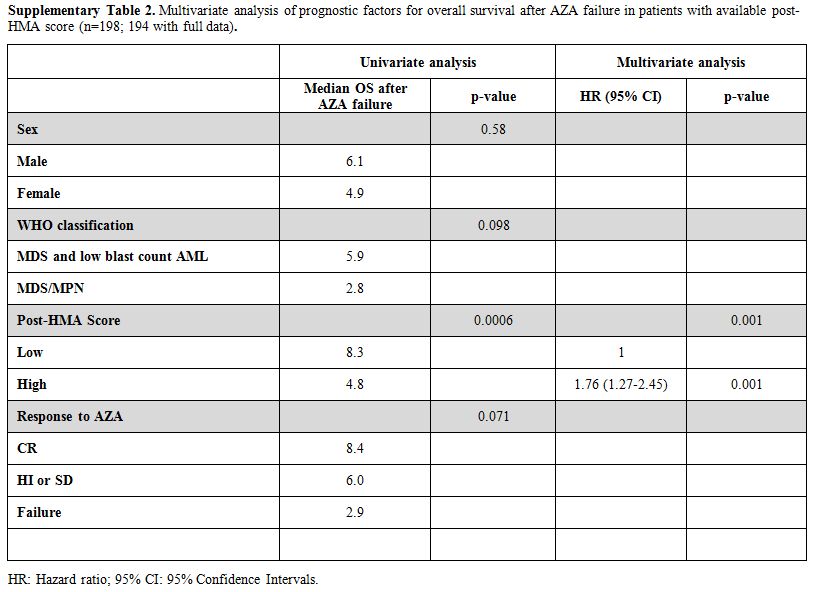
The median time to AZA discontinuation was 7.5 months (95% CI: 6.5–8.5) with 43 (13.2%) patients still receiving AZA at the time of analysis. The median OS from AZA failure (n=252), defined as AZA intolerance, no response after at least 4 cycles along with AZA intolerance, progressive disease or death while on treatment, and loss of response, was 5.6 (95% CI: 4.8–6.3) months, similar to the one reported in other studies.[2,3] Progressive disease while on treatment (n=77, 28%) and AZA intolerance (n=88, 31%) were the most common causes of AZA failure, followed by loss of an initial response (n=41, 15%) and no response after 4 cycles (n=25, 9%). Median OS after AZA failure was comparable for all of the above causes (p=0.1, Figure 2), indicating that the diverse pathobiology behind AZA failure does not influence the outcome and rather typical clinical parameters at the time of AZA failure, as those captured by the post-HMA model, determine patient survival. However, the 20% rate of early discontinuation and 7% rate of early death, i.e., occurring before cycle 4, underline the considerable toxicity of AZA in real-life settings, highlighting the need for early predictive factors to avoid a costly, ineffective and potentially even harmful treatment.
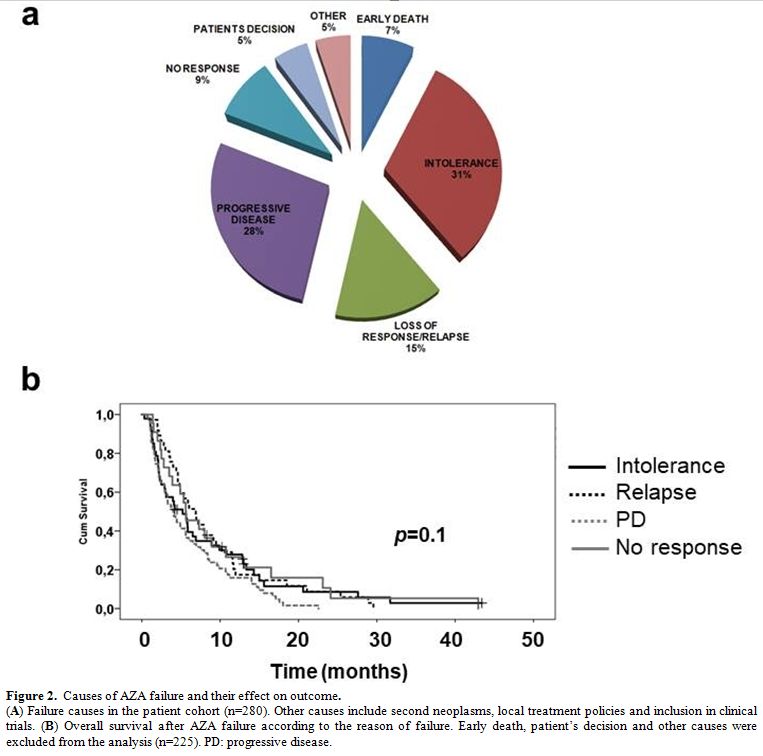 |
Figure 2. Causes of AZA failure and their effect on outcome. (A) Failure causes in the patient cohort (n=280). Other causes include second neoplasms, local treatment policies and inclusion in clinical trials. (B) Overall survival after AZA failure according to the reason of failure. Early death, patient’s decision and other causes were excluded from the analysis (n=225). PD: progressive disease. |
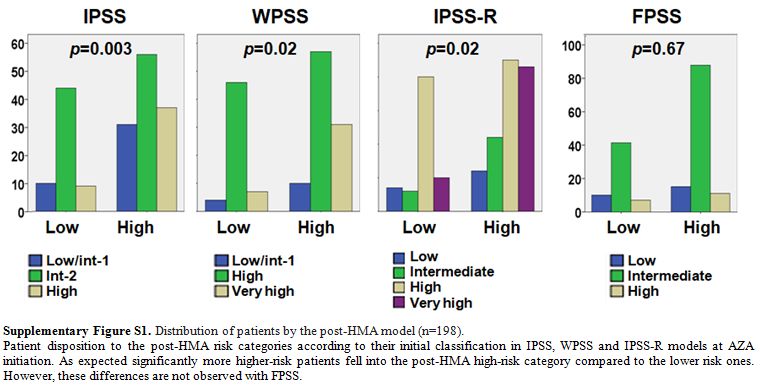
The post-HMA model4 was applicable in 198 patients (Figure 1B); 64 patients (32.5%) were classified as low and 134 (67.5%) as high risk, with a significant difference in median OS after AZA failure (8.3, 95% CI: 5.8–10.8 vs. 4.8, 95% CI: 3.7–5.9 months respectively, p<0.001). Eight out of 9 patients who proceeded to allogeneic transplantation were classified as low and only one as high risk, whereas even after censoring these patients at the time of transplantation, the median OS of the two groups remained identical (data not shown). In multivariate analysis, only the post-HMA model retained its independent predictive value (supplementary Table 2). Of note, our cohort included a considerable proportion of patients categorized as a low/intermediate-1 risk by IPSS (23.6%) at AZA initiation. The reported median OS after the failure of AZA in patients with IPSS low/int-1-risk score is 17 months.[9,10] By contrast, the median OS after AZA failure in our cohort of IPSS lower risk patients (n=54) was only 4.7 (95% CI: 1.6–7.8) months similar to one of the high-risk patients (n=172, Figure 1B). Though not easily interpretable, this inconsistency may be attributable to selection biases due to clinical judgment in real-life settings, i.e., administration of AZA mainly in poor prognosis, multi-treated patients. Indeed, at AZA initiation, only 24/75 (32%) of IPSS lower-risk patients were categorized as low risk by IPSS-R and 13/57 (23%) by FPSS. In addition, at the time of HMA failure 31/41 (76%) of the evaluable IPSS lower risk patients fell into the post-HMA high risk category, although, as expected, significantly more IPSS, WPSS and IPSS-R higher risk patients were classified as high risk by the post-HMA model (supplementary Figure S1).
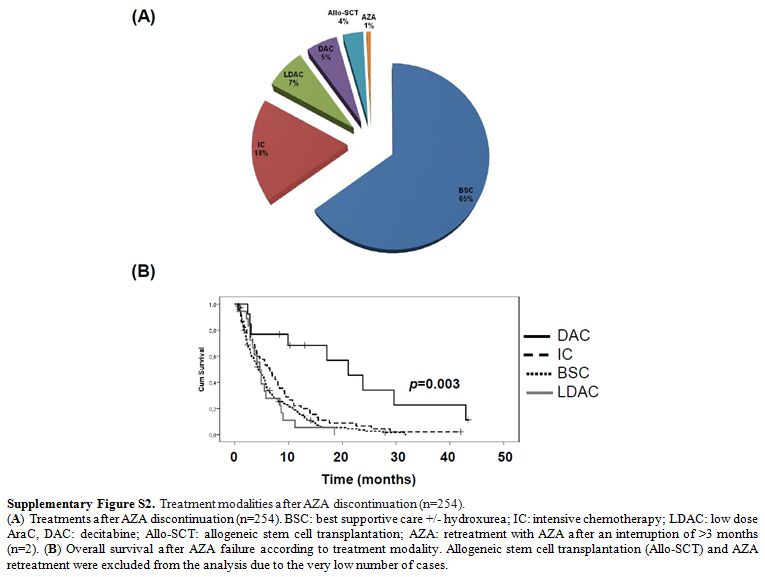
After AZA discontinuation, most patients were treated with supportive care, and only 9 patients proceeded to allo-SCT. Median OS after AZA failure was identical among patients treated with best supportive care, low dose AraC and intensive chemotherapy (p=0.22), whereas 14 patients treated with decitabine showed significantly improved mOS compared to all other treatments (21.1, 95% CI: 12–30.1 months, p=0.003, Supplementary Figure S2). Regarding the above patients, 5/11 evaluable cases were low and 6/11 high risk by post-HMA, whereas 4 discontinued AZA because of relapse after an initial response, 2 for disease progression, 2 for toxicity, 2 for failure to achieve a response after 4 cycles and one by his own decision. The overall response rate with second-line decitabine after AZA failure ranges from 19.4% to 63%[2,11,12] and the median OS from 7.3 to 17.8 months, but the small patient cohorts, the heterogeneous definitions of AZA failure and the obvious selection biases, preclude the identification of predictive factors for response in decitabine. Therefore, though selected patients who failed AZA may benefit from second line decitabine, no solid recommendation can be made, also considering the toxicity and cost of decitabine treatment.
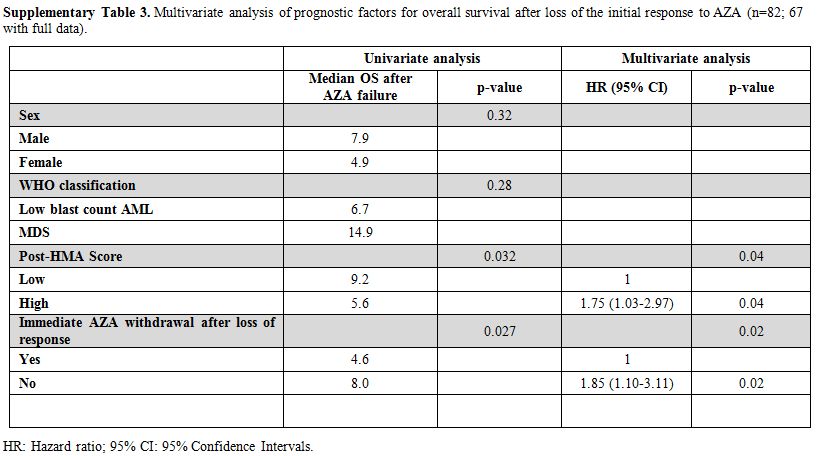
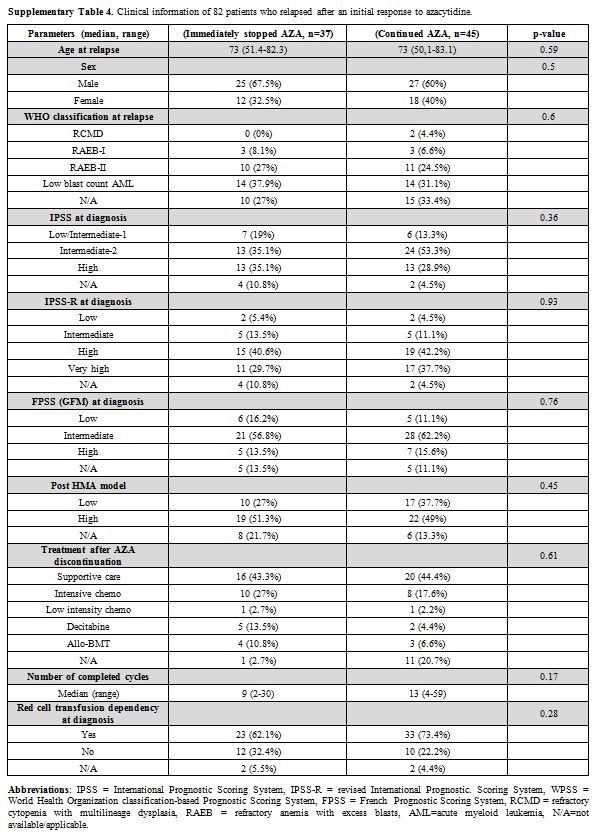
According to the latest International Working Group (IWG) criteria,[6] a hemoglobin drop of ≥1.5 g/dL or ≥50% decrement of maximum response levels of neutrophils or platelets signifies the loss of response. However, even large fluctuations in blood counts during AZA treatment can occasionally be observed in responding patients and, in the face of limited subsequent therapeutic options, many physicians are reluctant to immediately stop AZA simply only on the base of strictly defined loss of response. In our series, 45/82 patients, who continued AZA despite loss of response, had a significantly better OS (8.0 months, 95% CI: 5.5–10.5) compared to those (n=37) who stopped AZA immediately at loss of response (4.6 months, 95% CI: 1.5–7.9, p=0.027, Figure 1B). The decision to stop or not AZA when the response is lost according to the IWG criteria is subjected to bias, of course. However, patients who continued AZA had still significantly longer OS even when the analysis was adjusted for gender, disease subtype at the time of AZA discontinuation and the post-HMA model (p=0.02), though both patient groups received comparable therapies after AZA discontinuation (supplementary Tables 3 and 4). In line with these findings, our group has recently shown that patients with stable disease as best response benefited significantly by the continuation of AZA compared to the ones who stopped treatment.[13] By contrast, prolonged survival was recently reported in patients who stopped AZA or decitabine without disease progression, but the study cohort consisted mainly of IPSS low-risk patients, most of whom discontinued treatment for extra medical causes.[14]
In summary, in our large patient dataset, we confirmed the superior efficacy of FPSS and post-HMA models in predicting OS at AZA start and failure, respectively. However, our data also indicate that in real life settings, AZA failure is rather ill-defined, and physicians’ perceptions of the cause and timing of AZA discontinuation differ widely. Retrospective data are inherently susceptible to selection and analysis bias. Specifically for the setting of AZA failure, the highly diverse reasons of AZA discontinuation in our series emphasize that, since no uniform criteria for stopping AZA have been adopted,[15] any survival comparisons should be given with caution. Failure due to intractable toxicity and disease progression confers very poor outcome, while patients who lose the initial response may benefit from AZA continuation despite poor prognostic features, highlighting, on the one hand, the diversity of the resistance mechanisms to AZA and, on the other, the limitations of the applicability of prognostic models[16] and response criteria in everyday clinical practice.