Bent-Are Hansen1, Øystein Wendlebo2,3, Øyvind Bruserud4, Anette Lodvir Hemsing5, Knut Anders Mosevoll5 and Håkon Reikvam5,6.
1 Department of Medicine, Haraldsplass Deaconess Hospital, Bergen, Norway.
2 VID Specialized University, Faculty of Health, Bergen, Norway.
3 Department of Cardiology, Haukeland University Hospital, Bergen, Norway.
4 Department of Anesthesiology and Intensive care, Haukeland University Hospital, Bergen, Norway.
5 Department of Medicine, Haukeland University Hospital, Bergen, Norway.
6 Department of Clinical Science, University of Bergen, Bergen, Norway.
Corresponding
author: MD PhD Håkon Reikvam, Department of Clinical Science,
University of Bergen, Bergen, Norway. N-5021 Bergen, Norway. Tel. 55 97
50 00; Fax. 55 97 29 50. E-mail:
Hakon.Reikvam@med.uib.no
Published: January 1, 2019
Received: September 30, 2019
Accepted: December 17, 2019
Mediterr J Hematol Infect Dis 2020, 12(1): e2020009 DOI
10.4084/MJHID.2020.009
This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Acute
leukemias are a group of aggressive malignant diseases associated with
a high degree of morbidity and mortality. An important cause of both
the latter is infectious complications. Patients with acute leukemia
are highly susceptible to diseases due to factors related to the
disease itself, factors attributed to treatment, and specific
individual risk factors in each patient. Patients with
chemotherapy-induced neutropenia are at particularly high risk, and
microbiological agents include viral, bacterial, and fungal agents. The
etiology is often unknown in infectious complications, although
adequate patient evaluation and sampling have diagnostic, prognostic
and treatment-related consequences. Bacterial infections include a wide
range of potential microbes, both Gram-negative and Gram-positive
species, while fungal infections include both mold and yeast. A
recurring problem is increasing resistance to antimicrobial agents, and
in particular, this applies to extended-spectrum beta-lactamase
resistance (ESBL), Pseudomonas aeruginosa, methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus (VRE) and even carbapenemase-producing Enterobacteriaceae
(CPE). International guidelines for the treatment of sepsis in leukemia
patients include the use of broad-spectrum Pseudomonas-acting
antibiotics. However, one should implant the knowledge of local
microbiological epidemiology and resistance conditions in treatment
decisions. In this review, we discuss infectious diseases in acute
leukemia with a major focus on febrile neutropenia and sepsis, and we
problematize the diagnostic, prognostic, and therapeutic aspects of
infectious complications in this patient group. Meticulously and
thorough clinical and radiological examination combined with adequate
microbiology samples are cornerstones of the examination. Diagnostic
and prognostic evaluation includes patient review according to the
multinational association for supportive care in cancer (MASCC) and
sequential organ failure assessment (SOFA) scoring system.
Antimicrobial treatments for important etiological agents are
presented. The main challenge for reducing the spread of resistant
microbes is to avoid unnecessary antibiotic treatment, but without
giving to narrow treatment to the febrile neutropenic patient that
reduce the prognosis.
|
Introduction
Acute
leukemia is a group of highly malignant blood disorders characterized
by clonal growth of immature progenitor cells in the bone marrow. This
infiltration leads to severe thrombocytopenia, anemia and leukopenia,
and that makes fatal within a few weeks this disease if left untreated.
There are three major groups of acute leukemias; acute myeloid leukemia
(AML),[1] acute lymphocytic leukemia (ALL),[2] and on very rare occasions mixed phenotype acute leukemia (MPAL).[3]
The clinical presentation is often similar, although the treatment
protocols are different, and the diseases can only be cured by
intensive chemotherapy treatment, possibly in combination with
allogeneic hematopoietic stem cell transplantation (allo-HSCT).[1-3]
Infectious complications continue to be a significant cause of both
morbidity and mortality in acute leukemia patients. In the present
article, we review the current and update knowledge regarding
pathophysiology, epidemiology and etiology of infectious complications
in patients with acute leukemia. Finally, we discuss optimal approaches
to adequate diagnosis and discuss treatment options for this demanding
patient group.
Pathophysiology and Risk Factors
The
clinical susceptibility for infections among patients with
hematological malignancies is multifactorial. The risk of development
and the severity of infections are determinate by a complex interplay
between the pathogen and its virulence, and the degree of impaired
defense mechanisms of the host. The risk of infection can broadly be
divided into (i) disease-associated factors, (ii) patient-related
factors, and (iii) treatment-related factors (Figure 1).
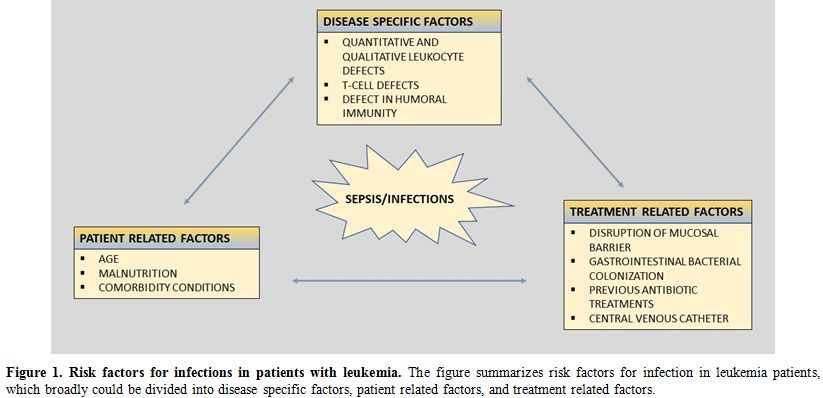 |
Figure
1. Risk factors for infections in patients with leukemia.
The figure summarizes risk factors for infection in leukemia patients,
which broadly could be divided into disease specific factors, patient
related factors, and treatment related factors. |
Disease-associated Factors.
In acute leukemia, normal bone marrow function is to more or less
extent, replaced by abnormal maturation and dysregulated proliferative
immature cells, resulting in neutropenia and impaired granulocyte
function.[1-3] It is well established that
quantitative reduction in circulating immune cells makes the organisms
more susceptibility for invasive infections.[4] Furthermore, immature myeloid cells have the potential to inhibit the antigen-specific T-cell response.[5]
The humoral immune system is also affected by the disease and its
treatment, so the majority of patients will have immunoglobulins'
deficiency. IgG and IgM being the most affected immunoglobulins, and
humoral defect immunity can also be present in patients achieving
complete remission.[6] Finally, the incidence and
severity of infections and sepsis are very different in AML patients
compared to ALL patients. Induction treatment induces in AML more
prolonged neutropenia, which favors infectious complications with early
deaths, significantly more frequent in AML patients compared to ALL
patients.[7-10]
Patient-related Factors.
Intrinsic properties related to the patient itself are also important
in the assessment of infection risk in patients with acute leukemia.
Age itself is a major risk for developing infectious complications
during the treatment of acute leukemia.[11] The natural function of the immune system declines by age,[12] as both the B- and T-cell function will be reduced with increasing age.[12] In addition, elderly patients are often frailer and have comorbidities affecting infection susceptibility,[11]
increasing the risk of both morbidity and mortality of the disease and
the treatment. Although studies have found that older patients are not
more susceptible to infections,[13] one must take
into account that older patients are often treated with milder and less
toxic chemotherapy regimens affecting infectious risk.[11] Age and comorbidity burden increase the risk for intensive care unit (ICU) admission,[14]
and severe comorbidity is a strong predictor for early death in acute
leukemia patients, death often caused by infectious complications.[15]
In
recent years, there has also been an increased focus on nutrition, and
undernourishment is considered a critical risk for severe infection
complications.[16] Nutritional problems are often
linked to the treatment of leukemia, as nausea, vomiting, and emesis
are common treatment side effects. Consequently, reduced food intake
and weight loss are often complementarities to the treatment, and
reduced nutritional intake increases the risk of serious infections.
Low initial body mass index (BMI) and more pronounced weight loss
during treatment courses are reliable prognostic indicators associated
with lower survival and both bacterial and fungal infections.[17]
Furthermore,
global challenges regarding the diagnostic and treatment of infectious
complications in acute leukemia patients are also important to take
into considerations. For example, for children treated for ALL, the
rates of infection-associated mortality are up to 10-times higher in
low- and middle-income countries than in high-income countries.[18]
This is due to several underlying factors such as shortage of trained
personnel, supplies, diagnostic tools, and adequate infrastructures as
well as undernourishment and risk of multiple drug-resistant organisms
(MDROs).[18] Also, in high-income countries,
socioeconomic status seems to be a risk factor for infection and early
complications in acute leukemia patients.[19]
Finally, lower early mortality is also registered in centers with
larger patients’ volume and more specialized cancer centers. It may
result from differences in the hospital or provider experience and
supportive care.[20,21]
Treatment-related Factors.
Treatment of acute leukemia requires intensive chemotherapy with high
dose drugs, often in a combination regimen, resulting in prolonged
neutropenia, often lasting for weeks.[1-3] The risk of developing more serious and complicated infections is clearly linked to the degree and duration of neutropenia.[4]
The risk of severe infections is not uniform among these patients, and
factors associated with increased susceptibility for infectious
complications include prolonged neutropenia,[22] use of salvage chemotherapy,[23] and relapsed disease.[24] However, other factors than the leukopenia itself are associated with infectious risk.
Mucosal
barriers separate self from non-self and are the first line of defense
against external pathogens. Epithelia at mucosal surfaces must allow
selective paracellular flux, and at the same time preventing the
passage of potentially infectious agents.[25]
Leukemia patients receiving cytotoxic therapy or radiotherapy will
experience mucosal barrier injury, often termed mucositis. The barrier
disruption will create an entrance point for resident microorganisms,
with the potential to cause bloodstream infections.[26]
Consequently, the infections are typical due to those opportunistic
pathogens that inhabit the skin, oral cavity, and the gastrointestinal
tract, rather than more conventional pathogens such as Streptococcus pneumonia (S. pneumonia) and Staphylococcus aureus (S. aureus).[27]
Furthermore,
gastrointestinal bacterial colonization will often be affected during
the treatment course of acute leukemia, both trough mucosal barrier
injuries, and the use of broad spectra antibiotics and other microbial
agents.[26,28] This will affect the
natural bacterial flora of the intestinal tract, often termed the
microbiota. Decreases in both oral and feces microbial diversity are
associated with the receipt of carbapenem antibiotics.[29] Furthermore, loss of microbial diversity throughout treatment is associated with the risk of infection[29] and with a higher risk of mortality in the setting of allo-HSCT.[30] Clostridium difficile
is clearly associated with the use of broad spectra antibiotics, and
the risk of clinical infections is increased among leukemia patients
and associated with increased mortality.[31] In addition, the use of antibiotics sets the patients for risk for colonization with MDROs.[32] Colonization with MDROs, especially Enterococcus faecalis (E. faecalis), Enterococcus faecium (E .faecium), and Stenotrophomonas maltophilia (S. maltophilia),
has been clearly associated with risk of infections and
non-relapse-related mortality in the setting of allo-HSCT in AML
patients.[33,34] Colonization in the intestine,
previous use of antimicrobial therapy, especially beta-lactams and
cephalosporins, and the total length of hospitalization, all increases
the risk of more for MDROs, including extended-spectrum beta-lactamase
resistance (ESBL)[32,35-38] Central
venous catheters (CVCs) are an essential tool for appropriate
management of patients with acute leukemia. However, CVCs are an
entrance port for bacteria into the bloodstream and a potential for
bacterial colonization. CVCs increase the risk for bloodstream
infections, and the infection risk is correlated with the numbers of
CVC manipulations. The patients are especially vulnerable to
gram-positive infections.[39] The rate of central-line associated bloodstream infections is estimated to 2/1000 catheter days,[40] and delaying CVC placement in acute leukemia does not affect the reduction of infectious risk.[41]
In contrast, antiseptic coating of intravascular catheters may be
effective in decreasing catheter-related colonization and subsequent
infections.[42] Early removal of CVCs should always be considered for leukemia patients with undocumented sepsis.[43]
Furthermore, in recent years the use of peripherally inserted central
catheters is increasing and is associated with a lower risk of
bloodstream infections.[44] A study from China in the
period 2011-2014 demonstrated that the risk of BSI in the use of
peripherally inserted central catheters in cancer patients was
0.05/1000 catheter days, and the overall risk of infections was
approximately 1/1000 catheter days.[44]
Taken
together, all factors related to one of these three conditions increase
the risk of infections in leukemia patients, and proper evaluation of
all these risk factors should be considered when evaluating leukemia
patients for prophylaxis and treatment of infectious complications.
Febrile Neutropenia and Sepsis
According
to the third international consensus definitions for sepsis and septic
shock, sepsis is defined as life-threatening organ dysfunction caused
by a dysregulated host response to infection.[45] Organ dysfunction is identified as an acute change in the sequential organ failure assessment (SOFA) score.[46]
Septic shock is defined as a subset within sepsis in which underlying
circulatory and cellular/metabolic abnormalities are profound enough to
increase the mortality risk substantially. Bacteremia is defined as the
growth of bacteria in blood cultures, although infections do not have
to be proven to diagnose sepsis at the onset. These criteria also
define sepsis in patients with acute leukemia. These patients are
especially prone to bacterial infections following chemotherapy due to
severe neutropenia,[47,48] and their cellular immune
defect represents an additional predisposition to infections to fungi,
parasites, and viruses. However, leukemic patients are at risk for
infectious diseases and can present altered symptoms and signs due to
an impaired inflammatory response. Thus a high index of suspicion is
warranted.
Clinical Presentation and Diagnosis
Leukemic
patients may present altered symptoms and signs for sepsis and
infections because of an impaired inflammatory response, thus
discovering an infection, and the likely focus might represent a major
challenge. However, sepsis should be suspected in patients presenting
typical signs and symptoms for infections[49]
including fever (core temperature >38°C), hypothermia (<36°C),
heart rate >90 beats per minute, tachypnea (>30 breaths per
minute), altered mental status, significant edema or positive fluid
balance (>20 ml/kg over 24 hours), or hyperglycemia (plasma glucose
>110 mg/dl or 7.7 mmol/l) in the absence of diabetes. Besides, one
should be aware of organ-specific symptoms associated with infectious
diseases such as respiratory symptoms (cough, rhinorrhea, and
respiratory distress), gastrointestinal symptoms (nausea, vomiting,
diarrhea, and abdominal pain), and consciousness disturbance which all
should lead to further diagnostic work-up. Notably, mucositis and
cutaneous signs such as rash, local heat, swelling, exudate,
fluctuation, or ulceration can manifest infectious diseases in the
leukemic patient.
These latter signs will determine the likely
source of infection and the status of the organ function. The
Multinational Association for Supportive Care in Cancer (MASCC)-score,
Talcott's classification and the clinical index of stable febrile
neutropenia (CISNE) tool could help the assessment of the patients'
risk for developing a serious infection in patients with febrile
neutropenia.[50] MASCC-score index of <21
indicates a low risk, and the patient could be considered for
outpatient treatment with oral antibiotics. With high risk
(MASCC>21) or clinical suspicion of sepsis, the patient should
always be admitted to the hospital.[50] However, it is important to be
aware that only a minority of the patients (28%) in the original
MASCC-cohort were patients with acute leukemia.[51]
Direct comparison between CISNE and MASCC-score demonstrates that CISNE
gives a more specific identification of low-risk patients, although
with lower certainty in patients with acute leukemia.[52]
The 2016 3.0 sepsis definition recommended qSOFA as a screening tool
for patients with suspected sepsis. qSOFA has so far shown inferior
sensitivity compared to MASCC-score for risk assessment for sepsis
development in neutropenic patients.[53,54] Cautious
use of scoring systems, and still be clinical vigilant is important, as
more validation of these scoring systems are needed, also in
leukemia-cohorts.
Hemodynamic parameters can indicate organ
dysfunctions and sepsis development; arterial hypotension (systolic
blood pressure <90 mmHg, mean arterial pressure <70 mmHg, or a
systolic blood pressure decrease of >40 mmHg in adults or <2
standard deviations (SD) below normal for age), mixed venous oxygen
saturation >70%, cardiac index >3.5 l/min/m2, arterial hypoxemia (PaO2/FiO2<300), and acute oliguria (urine output <0.5 ml/kg/h or 45 ml for at least 2 h).
Laboratory testing helps estimate the severity of the infection and may indicate the source of infection.[49] Inflammatory markers indicating sepsis are leukocytosis (white cell counts (WBC) >12 x 109/l), leukopenia (WBC <4 x 109/l),
normal white cell counts with >10% of immature forms, and plasma
C-reactive protein (CRP) or procalcitonin >2 SD above the normal
value/range. Organ dysfunction can also easily be verified in
laboratory testing including creatinine increase ≥0.5 mg/dl,
coagulation abnormalities (international normalized ratio (INR) >1.5
or activated partial thromboplastin time (APTT) >60 seconds),
thrombocytopenia (platelet count <100 000/µl), and
hyperbilirubinemia (plasma total bilirubin >4 mg/dl or 70 µmol/l).
Hyperlactataemia (>3 mmol/l) can indicate decreased tissue
perfusion.
Appropriate cultures and Gram-stains (blood, sputum,
urine, fluids, and cerebrospinal fluid) are helpful to identify the
source of the infection and reveal the microbe. Blood cultures should
ideally be taken during fever and before the onset of antibiotics, and
are found positive in 40-60% of patients with septic shock. Positive
microbial findings can be crucial for the correct treatment of the
patient. The chest radiograph will aid in the diagnosis of pneumonia,
empyema, and acute lung injury. Abdominal ultrasound or computer
tomography (CT) scanning is indicated if abdominal sepsis is suspected,
and magnet resonance imaging (MRI) can help find infections in soft
tissues. Several factors can affect the outcome of FN, including the
patient's underlying disease, age, patients' clinical condition, number
of infectious foci, duration of the neutropenia, the onset of
antimicrobial therapy, geographical location, and local profile of
antimicrobial resistance.[55]
Despite advances
in antimicrobial treatment, bloodstream infections (BSIs) prolong
hospital stay, increase direct patient care costs, and cause
considerable mortality.[56,57] In neutropenic patients with fever of unknown origin, the attack rate for BSI is 11%–38%.[58]
Previous studies showed that infections were the cause of death for
50%-80% of acute leukemia patients, and for 50% of patients with
lymphoma and solid tumors.[59] In Figure 2,
we present an algorithm for the management of FN in leukemia patients,
including prognostic, diagnostic, and treatment decision work
up.
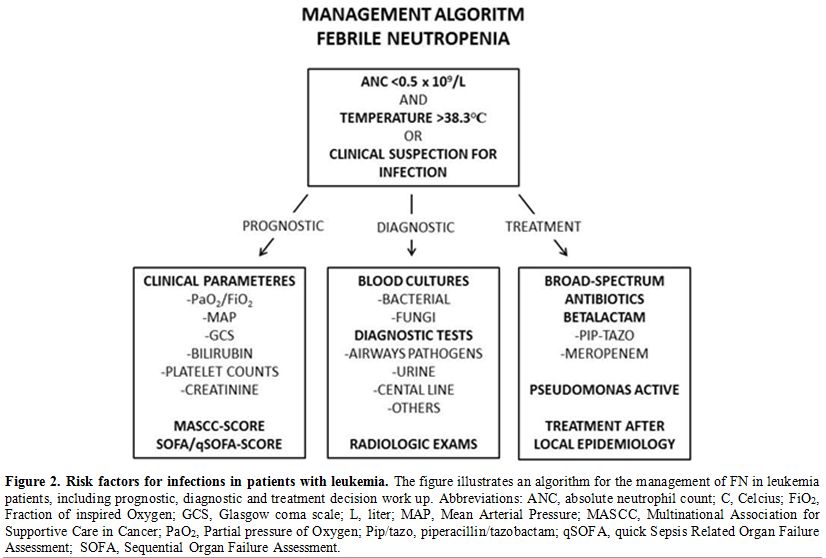 |
Figure 2. Risk factors for infections in patients with leukemia.
The figure illustrates an algorithm for the management of FN in
leukemia patients, including prognostic, diagnostic and treatment
decision work up. Abbreviations: ANC, absolute neutrophil count; C,
Celcius; FiO2, Fraction of inspired Oxygen; GCS, Glasgow coma scale; L,
liter; MAP, Mean Arterial Pressure; MASCC, Multinational Association
for Supportive Care in Cancer; PaO2, Partial pressure of Oxygen;
Pip/tazo, piperacillin/tazobactam; qSOFA, quick Sepsis Related Organ
Failure Assessment; SOFA, Sequential Organ Failure Assessment. |
Bacterial Etiology
Infectious
complications in patients with hematological malignancies occur most
frequently in patients with chemotherapy-induced cytopenia following
intensive chemotherapy,[60,61] and FN is most common in AML patients. The etiology is often unknown at the onset of infection.[62]
Knowledge of the prevalence of causative bacteria in neutropenic
patients with fever is important as infections can rapidly progress,
and FN patients can become hemodynamically unstable, as prompt and
rapid onset of adequate antimicrobial treatment within one hour is
recommended.[63,64] There are considerable site- and
region-specific differences in the incidence of resistant organisms
such as methicillin-resistant S. aureus
(MRSA) and vancomycin-resistant enterococcus (VRE). These local
differences may impact the initial choice of empiric antibiotic
therapy. Therefore, knowledge of the general and local epidemiology and
resistance profiles is of paramount importance in the optimal treatment
of febrile neutropenia.[65,66] The most frequent bacteria causing infections in acute leukemia patients are summarized in Table 1.[67-84]
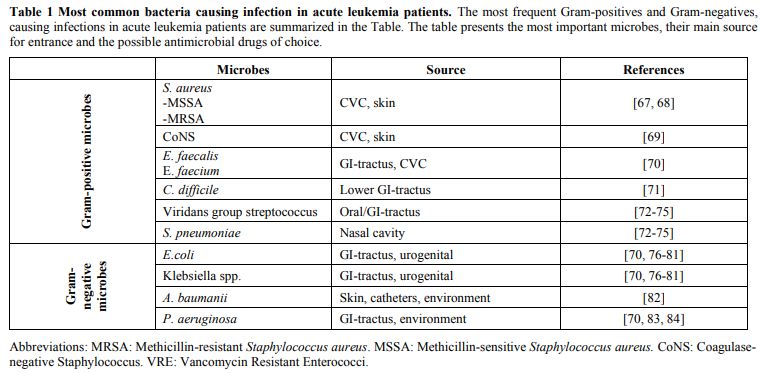 |
Table 1. Most common bacteria causing infection in acute leukemia patients.
The most frequent Gram-positives and Gram-negatives, causing infections
in acute leukemia patients are summarized in the Table. The table
presents the most important microbes, their main source for entrance
and the possible antimicrobial drugs of choice. |
Previous studies have documented bloodstream infections in 15–38% of patients with hematological malignancies.[62,85-87]
In Europe and the US, Gram-negative organisms were the most predominant
pathogens during the 1970s and the 1980s, followed by a shift toward
Gram-positive organisms.[86] In 2000, 76% of all BSI
in the US was associated with Gram-positive microbes, of which
coagulase-negative staphylococci (CoNS), viridans streptococci and
enterococci were the most frequently isolated pathogen.[87] Recently, a number of reports show a tendency towards an increase of Gram-positive bacteremia.[62,85-87]
This is usually attributed to the increasing use of indwelling CVCs and
the use of fluoroquinolone (FQ) prophylaxis, which suppresses the
aerobic Gram-negative organisms of the gastrointestinal tract.
Mortality is lower in patients with Gram-positive bacteremia than in
patients with Gram-negative bacteremia.[86] Epidemiological studies of BSI rank Gram-negative rods with Escherichia coli (E. coli) as the most frequently isolated pathogen.[86] More recently, the increased incidence of MDROs, such as Gram-negative Enterobacteriaceae, has been the scope of several papers.[88,89]
Gram-negative bacteria are reported as MDROs if not susceptible to at
least three of the following antimicrobial categories: antipseudomonal
penicillins, cephalosporins, carbapenems, aminoglycosides or FQs.[90] In several European countries,> 10% of invasive infections caused by E. coli were due to extended-spectrum beta-lactamases (ESBL).[66,91] Pseudomonas aeruginosa (P. aeruginosa)
is a Gram-negative pathogen associated with high mortality and accounts
for approximately 5-10% of BSI in hematological patients.[92] P aeruginosa
is characterized by several resistance mechanisms; (i) intrinsically
resistant to antimicrobial agents due to low permeability of its cell
wall, (ii) genetic capacity to express a vast repertoire of resistance
mechanisms, (iii) become resistant through mutations in regulative
resistance genes, and (iv) acquire additional resistance genes from
other organisms via plasmids, transposons and bacteriophages.[93]
Carbapenem resistance is reported as high as 3-51% in different geographical regions of Europe.[91] Acinetobacter
has emerged as a significant cause of health-care-associated infection
in critically ill and immunocompromised patients. Mortality rank
between 17-50% and Acinetobacter baumannii (A. baumannii) is estimated to be responsible for about 2-12% of BSI.[91] Oral mucositis, use of CVC and FQ prophylaxis increase the risk of Gram positive BSI. The most frequent isolated pathogen is staphylococcus spp, dominated by CoNS that accounts for about 25%-33% of all BSI.[94,95] The more virulent, S. aureus is responsible for only a smaller proportion of infections, accounting for about 5% of BSI.[86] The incidence of methicillin resistance is higher in CoNS than in S. aureus,
the median resistance rate of 80% and 56% respectively, and >60% of
European centers reporting more than 50% methicilline-resistance in
CoNS.[91,92]
Enterococcus spp. is now the third
most frequent group of pathogens in BSI and affects 10-12% of
transplant patients. Many centers report a shift from E. faecalis to E. faecium,
the latter being frequently resistant to ampicillin and demonstrate
increasing resistance to vancomycin (10.4% in 2014 and 14.9% in 2017).[96] The mortality rate is high, and in one study from a transplant center in the US, they found 30-day mortality of 38%.[97]
Noteworthy, enterococcus spp. in general have low virulence, and BSI
with enterococcus spp. have been clearly associated with severe
comorbidity, and their direct impact on mortality remains unclear.[96,98]
The
frequency of viridans streptococci in BSI of neutropenic patients with
cancer has significantly increased over the last 10–15 years and now
accounts for approximately 5% [87,99]
Risk factors in this patient population include severe neutropenia,
oral mucositis, administration of high-dose cytosine arabinoside, and
concomitant use of antimicrobial prophylaxis with either
trimethoprim-sulfa or an FQ. Viridans streptococci may contribute to
acute respiratory distress syndrome; in some studies, mortality rates
of 10% have been reported.[100]
Treatment of Bacterial Infections
FN
is a medical emergency, and early identification followed by diagnostic
blood cultures and prompt administration of appropriate intravenous
antibiotics remains the cornerstones in the initial management.
Harvesting microbiological cultures and source control obtained by
removal or drainage of the infected foci is mandatory. Empiric
antibiotic treatment should be started within the first hour after the
clinical suspicion is raised, according to guidelines for neutropenic
fever and sepsis.[50] When a causative microbe is
diagnosed, a more targeted antibiotic treatment could be possible,
resulting in more specific and less broad-spectrum antimicrobial
therapy. The main antibiotics and their characteristics are presented
in Table 2.[50,67,68,70,71,73-81,101-109]
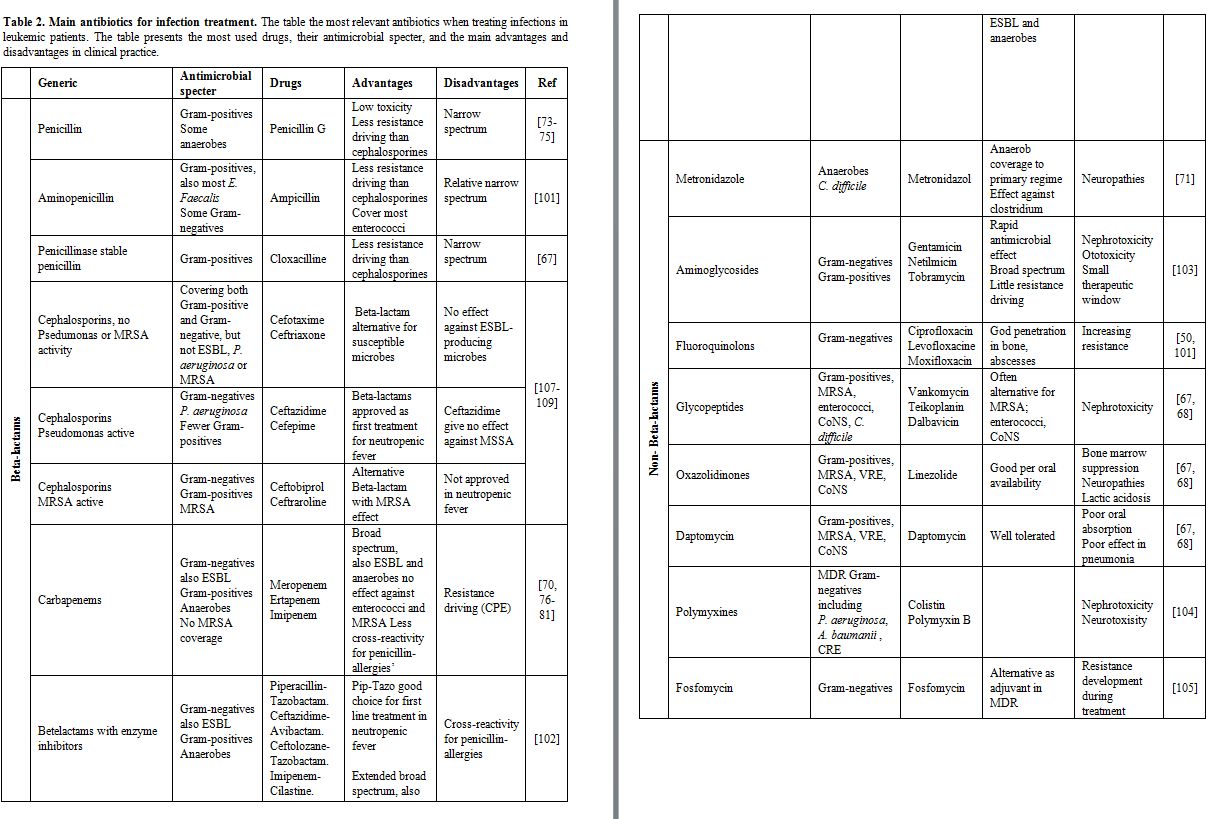 |
Table 2. Main antibiotics for infection treatment.
The table the most relevant antibiotics when treating infections in
leukemic patients. The table presents the most used drugs, their
antimicrobial specter, and the main advantages and disadvantages in
clinical practice. |
Adjuvant
sepsis-treatment as fluids therapy is important in sepsis treatment,
although secondary to antibiotic treatment and adequate source control.[110]
However, optimization of hemodynamically unstable patients, including
volume support supplemented with a vasopressor, inotropic and
transfusion of red blood cells (RBCs) in case of persistent
hypo-perfusion has the potential to reduce morbidity and mortality and
can prolong survival and improve quality of life.[45,111]
International recommended empiric treatment of neutropenic fever. International recommended empiric treatment for FN is initial broad covering with pseudomonas acting beta-lactam antibiotic.[50,81,90,112,113]
In cases of septic shock, guidelines recommend two Gram-negative acting
antibiotics, usually a beta-lactam and an aminoglycoside. Traditionally
a cephalosporin or piperazillin-tazobactam is recommended, although
this is challenged by the rapid spread of MDROs making carbapenem
treatment necessary.[70,76,77] This is, however, not only the case, as other treatment narrower antibacterial spectra are used in some centers.[90]
The emergence of carbapenemase-producing Enterobacteriaceae (CPE) also
makes the carbapenems less secure choice in several parts of the world.[78-81]
Escalation or de-escalation strategies are the two main approaches for
treatment, depending on the clinical condition of the patient (Table 3).[50,81,90,112,113]
In an escalation strategy, treatment is initiated with less broad
coverage, although escalation is performed if the patient responds
inadequately to the initial treatment. With de-escalation strategy,
broader antimicrobial therapies initiate the treatment, and if the
patient’s condition improves de-escalation is performed. Both
strategies depend on the correction of treatment after appropriate
microbiology results. With the rapid increase of MDROs, all centers
treating leukemia patients should carefully follow and monitor for
emerging resistant microbes and use the most appropriate treatment,
given local epidemiology.
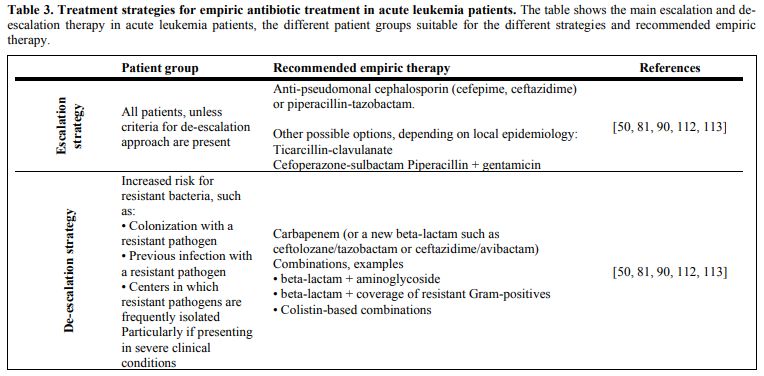 |
Table 3. Treatment strategies for empiric antibiotic treatment in acute leukemia patients.
The table shows the main escalation and de-escalation therapy in acute
leukemia patients, the different patient groups suitable for the
different strategies and recommended empiric therapy. |
Guidelines
used for febrile neutropenia are based on best available data, and a
challenge is that studies for febrile neutropenia are usually not
specific for leukemia. In Table 4,
we have indicated the main population in the studies supporting the
current guidelines. Because patients with solid tumors show different
phenotypes and different etiology, direct interpretation from these
studies should be careful. We have emphasized the description of the
microbiological etiology in the previous section because the suspected
pathogenic microbe is decisive when starting treatment. However, both
the microbiology and health organization varies in different countries,
regions and departments. Monitoring the local microbiology and
correction of local guidelines, and always try to choose the lesser
resistance driving treatment alternative is important. Recommendations
given in the next section reflect this, where the treatment of
different resistant microbes is described.
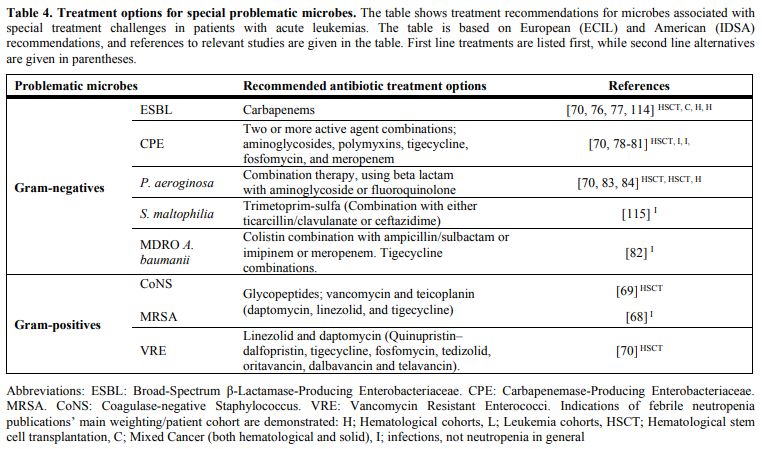 |
Table 4. Treatment options for special problematic microbes.
The table shows treatment recommendations for microbes associated with
special treatment challenges in patients with acute leukemias. The
table is based on European (ECIL) and American (IDSA) recommendations,
and references to relevant studies are given in the table. First line
treatments are listed first, while second line alternatives are given
in parentheses. |
Different local resistance patterns require adaptations of empirical treatment.
When a specific pathogen is identified, the treatment should be
corrected according to resistance as long as the microbiology result is
clinically plausible.[81] Before a definitive
resistance pattern is given, one will direct treatment after the local
resistance patterns for the identified microbe. Relevant antibiotic
treatment for unique problematic microbes based on the latest European
and American guidelines are presented in Table 4.[68-70,76-84,114,115]
The first choice for treating ESBL is carbapenems, beta-lactams with a time-dependent bactericide effect.[70,76,77] Aminoglycosides might also have an effect, although many ESBL-strains harbor resistance to aminoglycosides.[92]
Aminoglycosides have a concentration-dependent bactericide effect
depending on peak-concentration and a rapid bactericide effect, in
addition, to being synergistic to beta-lactams.[103]
CPE requires a combination of at least two antibiotics.[78-81]
The choices are limited and include high dose prolonged meropenem,
aminoglycosides, polymyxins, tigecyclin and fosfomycin, depending on
the resistance pattern. A high dose of meropenem increases the risk for
side effects; nephrotoxicity of aminoglycosides and polymyxins could be
challenging, while resistance development during treatment is a
significant disadvantage for tigecyclin and fosfomycin.
P. aeruginosa
is often susceptible to pseudomonas active cephalosporines and
piperazillin/tazobactam, although it will often develop resistance
during treatment.[70,83,84]
Meropenem will also be a suitable choice, and double coverage with
additional aminoglycoside should be considered, especially in unstable
patients and if anti-pseudomas drugs are previously used.[116]
Tobramycin is the recommended aminoglycoside, as high dose gentamycin
no longer is regarded as sufficient even with dosages of 7mg/kg.
Gentamycin is now proposed to be removed from The European Committee on
Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoints for
Pseudomonas spp.
MDRO A. baumani will often be challenging to treat and represents a major challenge in the treatment of leukemia patients if present.[82]
CoNS
are frequently found in catheter infection and BSI. Although not always
very virulent, CoNS might be difficult to treat due to resistance.[69]
Vancomycin is often the first treatment of choice, although treatment
has to be corrected after susceptibility-pattern. Cloxacilline,
daptomycin, linezolid, and tigecycline are possible alternatives.
The
MRSA incidence is varying from region to region, and coverage for MRSA
empirically should be considered according to local incidence.[68]
MRSA could be treated with vancomycin and daptomycin, although newer
MRSA-active cephalosporins have been developed. Other alternatives are
linezolid and tigecycline.
VRE are not very virulent but have a difficult susceptibility-pattern.[70]
Alternative treatments include linezolid and daptomycin. Alternatives
are quinupristin–dalfopristin, tigecycline, fosfomycin, tedizolid,
oritavancin, dalbavancin and telavancin.
The net antibiotic
consumption in society, both for human and animal use is one of the
most important predictors for the spread of antibiotic resistance.[117]
Acute leukemia patients are maybe the most vulnerable of all patients,
and among the individuals that easiest acquire resistant microbes due
to their immunocompromised state.[70] Acute leukemia
patients are in need of broad antibiotic coverage, although at the same
time, they are more vulnerable to side effects. The ideal treatment
should hence be exposure of antimicrobial agents with as narrow
antimicrobial specter for as short time as possible. Faster
microbiology service has made it possible to faster escalation or
de-escalation of the treatment, depending on the chosen treatment
strategy.
Norwegian antibiotic-recommendations for treatment of
neutropenic fever are penicillin and aminoglycoside contrary to
international recommendations.[72-75] International
studies show that aminoglycoside treatment increases the risk of
nephrotoxicity compared to beta-lactam treatment. However, studies from
countries with a low prevalence of MRDOs like Norway, indicate safety
with penicillin and aminoglycoside empiric treatment, given early
reconsideration and escalation when necessary.[72,74]
However, significant numbers of patients treated with this regime need
treatment alterations, although overall mortality is not increased
compared to other studies of FN.[72]
Invasive Fungal Infections
Invasive
fungal infections (IFI) represent a significant cause of treatment
failure in adults with acute leukemia, and the cumulative probability
of developing IFI after a diagnosis of acute leukemia has been
estimated to 11.1% at 100 days.[118] IFI is a major
cause of morbidity and mortality in patients with acute leukemia, and
patients treated for hematologic malignancies, and develop a
complicating IFI, have an estimated cause specific mortality due to IFI
of 35-38 %.[119,120] AML constitutes the hematologic
malignancy with the highest risk of associated IFI. In a report from
2006, Chamilos and coworkers found IFI in 314 of 1017 (31%) autopsies
of patients diagnosed with hematologic malignancies, of which only 25%
had been diagnosed with IFI while the patients were alive.[121]
Data
from previous studies have demonstrated; (i) the incidence of IFIs in
patients with hematologic malignancies has increased, (ii) over half of
IFIs emerge during the remission induction chemotherapy,[122] (iii) higher age, use of corticosteroid, ANC <0.1 X 109/L
at the time of IFI diagnosis, lack of recovery from aplasia, multiple
pulmonary localizations of infection and presence of indwelling
catheters all negatively influence outcome of IFI.[123,124]
The most frequently isolated yeast and mold spp. in patients with acute leukemias are presented in Table 5. The incidence of the most common fungal infections in patients with acute leukemia has changed in the last decade,[125]
and the incidence of yeast and mold infections show epidemiological
variations between regions, depending on the patient population, risk
factors and use of antifungal therapy. In certain geographical regions,
an association between the incidence of IFI, prevalent diseases, and
host factors exists. The occurrence of cryptococcal and Pneumocystis jirovecii (P. jirovecii) infections are reported in regions with a high prevalence of human immunodeficiency virus (HIV),[126,127] and diabetes is a risk factor for invasive mold infections.[128]
In mold infections, environmental factors predispose patients for
invasive infections, with hospital outbreaks linked to the use of
contaminated instruments and devices, Blastomycosis is associated with
occupational exposure (e.g., forest rangers) and recreational
activities (e.g., camping and fishing).[128,129]
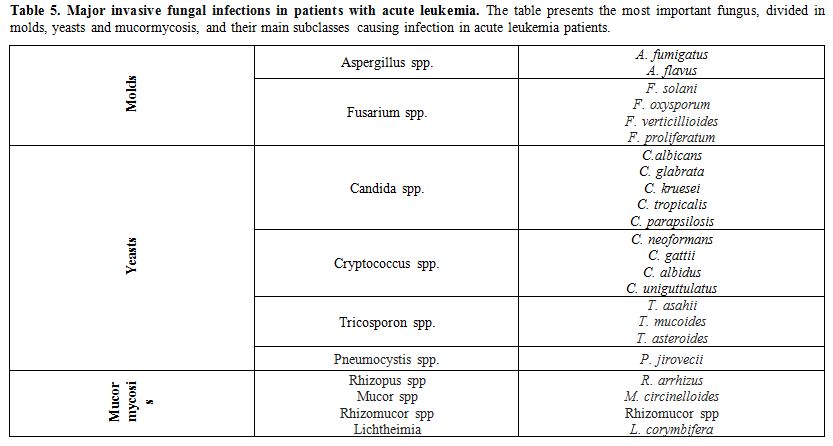 |
Table 5. Major invasive fungal infections in patients with acute leukemia.
The table presents the most important fungus, divided in molds, yeasts
and mucormycosis, and their main subclasses causing infection in acute
leukemia patients. |
Candida albicans (C. albicans)
was most frequently isolated in blood cultures in the '80s and
'90s.Since the introduction of fluconazole prophylaxis in hematology
units, there has been a gradual shift from C. albicans to non-C.albicans strains.[130] Candida spp. that are fluconazole-resistant (C. krusei) or susceptible–dose-dependent (C. glabrata) currently account for >80% candidiasis episodes in some hematology units.[131,132]
A
large concurrent surveillance study, Surveillance, and Control of
Pathogens of Epidemiological Importance (SCOPE), was used to examine
the secular trends in the epidemiology and microbiology of nosocomial
BSIs. They found Candida spp. to be the fourth most common isolated
pathogen causing BSIs, and C. albicans was the overall most frequently isolated pathogen.[133]
Invasive aspergillosis in patients with hematologic malignancies and in
patients undergoing allo-HSCT is still associated with high morbidity
and mortality.[122,134] There have also been an increase in non-Aspergillus fumigatus (A. fumigatus) spp., and other mold infections, i.e., Fusarium and Mucormycosis.[135] The emergence of C. auris
that show resistance to most known antifungals is still not frequent,
although it might present as a significant problem in the future.[136]
In
a study from Houston, incidence and risk factors for breakthrough
invasive mold infections (IMI) in AML patients receiving remission
induction chemotherapy were investigated. 17% of the patients had a
possible IMI and only 3.7% a proven diagnosis of IMI. The incidence of
proven or probable IMI per 1000 prophylaxis-days was not statistically
different between anti-Aspergillus azoles and micafungin. Older age and
relapsed/refractory AML diagnosis were associated with IMI on
multivariable analysis.[137] Introduction of
echinocandins and more recently introduced azoles may have contributed
to evolving the epidemiology of candidiasis, as incidences of both C. parapsilosis and C. tropicalis have increased in some treatment centers.[124,138]
Treatment of Fungal Infections
Fungal treatment could either be empiric, diagnostic driven or directed.[139]
Empiric therapy is used in centers where diagnostics are unavailable,
and include broad covering with antifungal treatment after persisting
fever for 5-7 days in neutropenic patients, despite antibiotic
treatment. The European Conference on Infections in Leukaemia
(ECIL)-guidelines recommend either caspofungin or liposomal
amphotericin B for empiric treatment.[140] In
diagnostic driven treatment, antifungal therapy is started if early
markers of fungal infections are presented. Markers for fungal
infection used in clinical practice include positive galactomannan
(GM)-test, positive beta-D-glucan (BDG)-test, PCR-screening, and
radiological examinations. Directed therapy is given patients with
proven fungal disease.
For invasive candidiasis, echinocandins
are first line treatment, although stepdown treatment to, i.e.
fluconazole, is recommended after susceptibility test results are
available.[141] Voriconazole, or now recently added isavuconazole, are first line treatment for invasive aspergillosis.[140]
Isavuconazole has shown non-inferiority compared to voriconazole,
although it has so far shown significantly fewer side effects.[142]
Treatment of mucormycosis is challenging and often includes surgical
debridement, if possible. Liposomal amphotericin B is first line
treatment.[140,143] P. jirovecii is usually treated with trimethoprim-sulfa as long as the treatment is tolerated.[106]
Other alternatives for the treatment of fungal infections, various
fungicides and their antifungal spectrum and important pharmacological
properties are presented in Table 6,[140-142,144] and treatment of particular problematic fungal infections are presented in Table 7.[106,140-143]
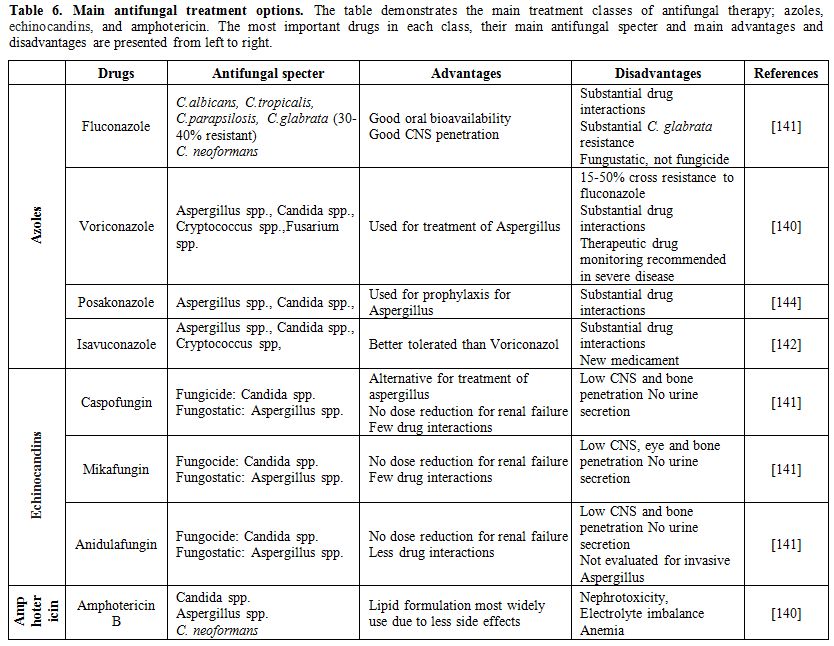 |
Table 6. Main antifungal treatment options.
The table demonstrates the main treatment classes of antifungal
therapy; azoles, echinocandins, and amphotericin. The most important
drugs in each class, their main antifungal specter and main advantages
and disadvantages are presented from left to right. |
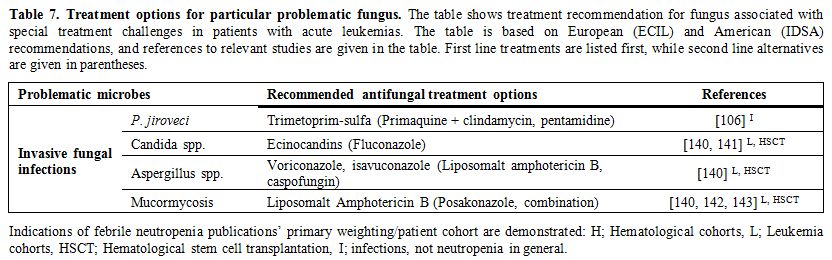 |
Table 7. Treatment options for particular problematic fungus.
The table shows treatment recommendation for fungus associated with
special treatment challenges in patients with acute leukemias. The
table is based on European (ECIL) and American (IDSA) recommendations,
and references to relevant studies are given in the table. First line
treatments are listed first, while second line alternatives are given
in parentheses. |
Prophylaxis of Bloodstream Infection and Fever During Neutropenia
Patients with acute leukemias are at risk of developing severe infections related to previously discussed factors (Figure 1). In the absence of preventive measures, 48-60% of the patients who became febrile have an established or occult infection.[145]The
use of antibiotic prophylaxis has been discussed widely in both Europe
and the US. According to European and American guidelines, FQs have
been recommended as prophylaxis during chemotherapy-induced neutropenia
in patients with expected neutropenic periods above seven days.[84]
In consideration of increased antibiotic resistance, the role of FQ
prophylaxis has been reevaluated. A meta-analysis based on two
randomized clinical trials and 12 observational studies published
between 2006 and 2012 concluded with a reduction of cases with BSI,
although without effect on overall mortality rate. Some of the studies
also found increased numbers of colonization or infections with MDROs.[84]The increased frequency of E. coli
resistance with increased FQ use is well documented and results mainly
form mutations in topoisomerase genes or changes in the expression of
efflux pumps. It may also be transmitted by plasmids, which can
transfer ESBL at the same time. The use of FQ has also been linked to
the proliferation of several other MDROs such as MRSA, VRE and C.
difficile.[146,147] However, patients at high risk
of FN should be considered for antimicrobial prophylaxis, including
patients with acute leukemias. The risk stratifications should be based
on patient characteristics, i.e., advanced age, performance status,
nutritional status, prior FN, comorbidity, and their underlying
leukemia.[148]In
contrast, most patients should not be considered for antifungal
prophylaxis, except those that are at risk for profound protracted
neutropenia, i.e. relapsed/refractory AML patients or patients
undergoing allo-HSCT. These latter patient groups should receive
prophylaxis with an oral azole or parenteral echinocandin.[148,149] Other Causes of Persistent Fever and Their Management
Occasionally
fever may be the only sign of an ongoing infection or non-infectious
process in patients with chemotherapy-induced neutropenia; other
decisive signs and symptoms of inflammation (erythema, swelling, pain,
infiltrates) may be absent. The febrile response is non-specific, and
concomitant use of antipyretic drugs (corticosteroids, paracetamol) may
suppress fever. As FN is a medical emergency, it is crucial to
accurately substantiate the differential diagnosis, as they require
different treatment strategies. Fever
in acute leukemia patients can also be attributed to by one of the
following reasons; (i) drug fever, (ii) tumor fever (iii) thrombosis,
or (iv) rheumatologic disorders. Drug fever is associated with
eosinophilia, acute interstitial nephritis, drug-induced hepatitis and
disappears rapidly after discontinuation of the particular drug.[150]
Tumor fever is one of the most common causes of non-infectious pyrexia
in febrile patients with malignancy, and may also occur in leukemia.[151] Thrombosis is always important to be aware of, as malignancy is a leading risk factor for the development of thrombosis.[152]
Rheumatologic disorders are also associated with the clinical
manifestations of a number of hematological and no-hematological
disorders and represent an important clue during the early diagnosis
and treatment of the cancer diseases.[153]
Conclusions
Acute
leukemias are a group of malignant blood disorders characterized by a
serious clinical course, and the only treatment with curative potential
is intensive chemotherapy, possibly combined with allo-HSCT. Infections
are important complications to both the diseases themselves and their
therapy. Thoroughly diagnostic workup, including microbiological
sampling, is the fundament of further handling and treatment.
Improvements in both treatment and prophylaxis against both bacterial
and fungal infections have helped to improve the treatment results for
acute leukemia patients. On the other hand, resistance development to
an increasing proportion of the antimicrobial agents we have available
is of considerable concern, and this, in turn, can lead to increased
morbidity and mortality among leukemia patients from infectious
complications. Therefore, physicians, who are treating this specific
patient group, must be carefully aware of this increasing problem and
make thorough considerations when choosing antimicrobial therapy. In
order to make leukemia treatment less toxic, and thereby reduce the
risk of serious infections, new searches for new and improved
antimicrobial agents are important to further improve treatment
outcomes among patients with acute leukemia.The dangerous, infectious complications and early mortality seem to be declining with time,[19]
since the diagnostic precision, prophylaxis and treatment have
increased over the past decades. However, this is currently challenged
by the increased risk of resistance development. References
- Döhner H, Weisdorf DJ, Bloomfield CD: Acute Myeloid Leukemia. N Engl J Med 2015, 373(12):1136-1152. https://doi.org/10.1056/NEJMra1406184 PMid:26376137
- Terwilliger
T, Abdul-Hay M: Acute lymphoblastic leukemia: a comprehensive review
and 2017 update. Blood Cancer J 2017, 7(6):e577. https://doi.org/10.1038/bcj.2017.53 PMid:28665419 PMCid:PMC5520400
- Khan
M, Siddiqi R, Naqvi K: An update on classification, genetics, and
clinical approach to mixed phenotype acute leukemia (MPAL). Ann Hematol
2018, 97(6):945-953. https://doi.org/10.1007/s00277-018-3297-6 PMid:29546454
- Bodey
GP, Buckley M, Sathe YS, Freireich EJ: Quantitative relationships
between circulating leukocytes and infection in patients with acute
leukemia. Ann Intern Med 1966, 64(2):328-340. https://doi.org/10.7326/0003-4819-64-2-328 PMid:5216294
- Almand
B, Clark JI, Nikitina E, van Beynen J, English NR, Knight SC, Carbone
DP, Gabrilovich DI: Increased production of immature myeloid cells in
cancer patients: a mechanism of immunosuppression in cancer. J Immunol
2001, 166(1):678-689. https://doi.org/10.4049/jimmunol.166.1.678 PMid:11123353
- Ashman
LK, Drew PA, Toogood IR, Juttner CA: Immunological competence of
patients in remission from acute leukaemia: apparently normal T cell
function but defective pokeweed mitogen-driven immunoglobulin
synthesis. Immunol Cell Biol 1987, 65 ( Pt 2):201-210. https://doi.org/10.1038/icb.1987.22 PMid:2956185
- Biswal
S, Godnaik C: Incidence and management of infections in patients with
acute leukemia following chemotherapy in general wards.
Ecancermedicalscience 2013, 7:310.
- Czyzewski
K, Galazka P, Fraczkiewicz J, Salamonowicz M, Szmydki-Baran A,
Zajac-Spychala O, Gryniewicz-Kwiatkowska O, Zalas-Wiecek P,
Chelmecka-Wiktorczyk L, Irga-Jaworska N et al: Epidemiology and outcome
of invasive fungal disease in children after hematopoietic cell
transplantation or treated for malignancy: Impact of national programme
of antifungal prophylaxis. Mycoses 2019, 62(11):990-998. https://doi.org/10.1111/myc.12990 PMid:31429997
- Hale
KA, Shaw PJ, Dalla-Pozza L, MacIntyre CR, Isaacs D, Sorrell TC:
Epidemiology of paediatric invasive fungal infections and a
case-control study of risk factors in acute leukaemia or post stem cell
transplant. Brit J Haematol 2010, 149(2):263-272. https://doi.org/10.1111/j.1365-2141.2009.08072.x PMid:20096013
- Styczynski
J, Czyzewski K, Wysocki M, Gryniewicz-Kwiatkowska O,
Kolodziejczyk-Gietka A, Salamonowicz M, Hutnik L, Zajac-Spychala O,
Zaucha-Prazmo A, Chelmecka-Wiktorczyk L et al: Increased risk of
infections and infection-related mortality in children undergoing
haematopoietic stem cell transplantation compared to conventional
anticancer therapy: a multicentre nationwide study. Clin Microbiol
Infect 2016, 22(2):179 e171-179 e110. https://doi.org/10.1016/j.cmi.2015.10.017 PMid:26493843
- Ossenkoppele G, Lowenberg B: How I treat the older patient with acute myeloid leukemia. Blood 2015, 125(5):767-774. https://doi.org/10.1182/blood-2014-08-551499 PMid:25515963
- Muller L, Di Benedetto S, Pawelec G: The Immune System and Its Dysregulation with Aging. Subcell Biochem 2019, 91:21-43. https://doi.org/10.1007/978-981-13-3681-2_2 PMid:30888648
- Fanci
R, Leoni F, Longo G: Nosocomial infections in acute leukemia:
comparison between younger and elderly patients. New Microbiol 2008,
31(1):89-96.
- Halpern AB, Culakova E,
Walter RB, Lyman GH: Association of Risk Factors, Mortality, and Care
Costs of Adults With Acute Myeloid Leukemia With Admission to the
Intensive Care Unit. JAMA Oncol 2017, 3(3):374-381. https://doi.org/10.1001/jamaoncol.2016.4858 PMid:27832254 PMCid:PMC5344736
- Djunic
I, Virijevic M, Novkovic A, Djurasinovic V, Colovic N, Vidovic A,
Suvajdzic-Vukovic N, Tomin D: Pretreatment risk factors and importance
of comorbidity for overall survival, complete remission, and early
death in patients with acute myeloid leukemia. Hematology 2012,
17(2):53-58. https://doi.org/10.1179/102453312X13221316477651 PMid:22664041
- Tvedt
TH, Reikvam H, Bruserud O: Nutrition in Allogeneic Stem Cell
Transplantion--Clinical Guidelines and Immunobiological Aspects. Curr
Pharm Biotechnol 2016, 17(1):92-104. https://doi.org/10.2174/138920101701151027163600 PMid:26420050
- Baumgartner
A, Zueger N, Bargetzi A, Medinger M, Passweg JR, Stanga Z, Mueller B,
Bargetzi M, Schuetz P: Association of Nutritional Parameters with
Clinical Outcomes in Patients with Acute Myeloid Leukemia Undergoing
Haematopoietic Stem Cell Transplantation. Ann Nutr Metab 2016,
69(2):89-98. https://doi.org/10.1159/000449451 PMid:27639391
- Caniza
MA, Odio C, Mukkada S, Gonzalez M, Ceppi F, Chaisavaneeyakorn S,
Apiwattanakul N, Howard SC, Conter V, Bonilla M: Infectious
complications in children with acute lymphoblastic leukemia treated in
low-middle-income countries. Expert Rev Hematol 2015, 8(5):627-645. https://doi.org/10.1586/17474086.2015.1071186 PMid:26211675
- Ho
G, Jonas BA, Li Q, Brunson A, Wun T, Keegan THM: Early mortality and
complications in hospitalized adult Californians with acute myeloid
leukaemia. Brit J Haematol 2017, 177(5):791-799. https://doi.org/10.1111/bjh.14631 PMid:28419422 PMCid:PMC5444943
- Ho
G, Wun T, Muffly L, Li Q, Brunson A, Rosenberg AS, Jonas BA, Keegan
THM: Decreased early mortality associated with the treatment of acute
myeloid leukemia at National Cancer Institute-designated cancer centers
in California. Cancer 2018, 124(9):1938-1945. https://doi.org/10.1002/cncr.31296 PMid:29451695 PMCid:PMC6911353
- Alvarez
EM, Malogolowkin M, Li Q, Brunson A, Pollock BH, Muffly L, Wun T,
Keegan THM: Decreased Early Mortality in Young Adult Patients With
Acute Lymphoblastic Leukemia Treated at Specialized Cancer Centers in
California. J Oncol Pract 2019, 15(4):e316-e327. https://doi.org/10.1200/JOP.18.00264 PMid:30849003
- Gill
S, Carney D, Ritchie D, Wolf M, Westerman D, Prince HM, Januszewicz H,
Seymour JF: The frequency, manifestations, and duration of prolonged
cytopenias after first-line fludarabine combination chemotherapy. Ann
Oncol 2010, 21(2):331-334. https://doi.org/10.1093/annonc/mdp297 PMid:19625344
- Wolach
O, Itchaki G, Bar-Natan M, Yeshurun M, Ram R, Herscovici C, Shpilberg
O, Douer D, Tallman MS, Raanani P: High-dose cytarabine as salvage
therapy for relapsed or refractory acute myeloid leukemia--is more
better or more of the same? Hematol Oncol 2016, 34(1):28-35. https://doi.org/10.1002/hon.2191 PMid:25689584
- Zajac-Spychala
O, Skalska-Sadowska J, Wachowiak J, Szmydki-Baran A, Hutnik L, Matysiak
M, Pierlejewski F, Mlynarski W, Czyzewski K, Dziedzic M et al:
Infections in children with acute myeloid leukemia: increased mortality
in relapsed/refractory patients. Leuk Lymphoma 2019:1-8.
- France MM, Turner JR: The mucosal barrier at a glance. J Cell Sci 2017, 130(2):307-314. https://doi.org/10.1242/jcs.193482 PMid:28062847 PMCid:PMC5278669
- van
der Velden WJ, Herbers AH, Netea MG, Blijlevens NM: Mucosal barrier
injury, fever and infection in neutropenic patients with cancer:
introducing the paradigm febrile mucositis. Brit J Haematol 2014,
167(4):441-452. https://doi.org/10.1111/bjh.13113 PMid:25196917
- Klastersky
J, Ameye L, Maertens J, Georgala A, Muanza F, Aoun M, Ferrant A,
Rapoport B, Rolston K, Paesmans M: Bacteraemia in febrile neutropenic
cancer patients. Int J Antimicrob Agents 2007, 30 Suppl 1:S51-59. https://doi.org/10.1016/j.ijantimicag.2007.06.012 PMid:17689933
- Kim
S, Covington A, Pamer EG: The intestinal microbiota: Antibiotics,
colonization resistance, and enteric pathogens. Immunol Rev 2017,
279(1):90-105. https://doi.org/10.1111/imr.12563 PMid:28856737 PMCid:PMC6026851
- Galloway-Pena
JR, Smith DP, Sahasrabhojane P, Ajami NJ, Wadsworth WD, Daver NG,
Chemaly RF, Marsh L, Ghantoji SS, Pemmaraju N et al: The role of the
gastrointestinal microbiome in infectious complications during
induction chemotherapy for acute myeloid leukemia. Cancer 2016,
122(14):2186-2196. https://doi.org/10.1002/cncr.3039 PMid:27142181 PMCid:PMC5574182
- Taur
Y, Jenq RR, Perales MA, Littmann ER, Morjaria S, Ling L, No D, Gobourne
A, Viale A, Dahi PB et al: The effects of intestinal tract bacterial
diversity on mortality following allogeneic hematopoietic stem cell
transplantation. Blood 2014, 124(7):1174-1182. https://doi.org/10.1182/blood-2014-02-554725 PMid:24939656 PMCid:PMC4133489
- Luo
R, Greenberg A, Stone CD: Outcomes of Clostridium difficile infection
in hospitalized leukemia patients: a nationwide analysis. Infect
Control Hosp Epidemiol 2015, 36(7):794-801. https://doi.org/10.1017/ice.2015.54 PMid:25801085
- Garcia-Vidal
C, Cardozo-Espinola C, Puerta-Alcalde P, Marco F, Tellez A, Aguero D,
Romero-Santana F, Diaz-Beya M, Gine E, Morata L et al: Risk factors for
mortality in patients with acute leukemia and bloodstream infections in
the era of multiresistance. PloS one 2018, 13(6):e0199531. https://doi.org/10.1371/journal.pone.0199531 PMid:29953464 PMCid:PMC6023133
- Scheich
S, Lindner S, Koenig R, Reinheimer C, Wichelhaus TA, Hogardt M, Besier
S, Kempf VAJ, Kessel J, Martin H et al: Clinical impact of colonization
with multidrug-resistant organisms on outcome after allogeneic stem
cell transplantation in patients with acute myeloid leukemia. Cancer
2018, 124(2):286-296. https://doi.org/10.1002/cncr.31045 PMid:28960264
- Scheich
S, Koenig R, Wilke AC, Lindner S, Reinheimer C, Wichelhaus TA, Hogardt
M, Kempf VAJ, Kessel J, Weber S et al: Stenotrophomonas maltophilia
colonization during allogeneic hematopoietic stem cell transplantation
is associated with impaired survival. PloS one 2018, 13(7):e0201169. https://doi.org/10.1371/journal.pone.0201169 PMid:30024969 PMCid:PMC6053200
- Cattaneo
C, Antoniazzi F, Tumbarello M, Skert C, Borlenghi E, Schieppati F,
Cerqui E, Pagani C, Petulla M, Re A et al: Relapsing bloodstream
infections during treatment of acute leukemia. Ann Hematol 2014,
93(5):785-790. https://doi.org/10.1007/s00277-013-1965-0 PMid:24288110
- Tanir
Basaranoglu S, Ozsurekci Y, Aykac K, Karadag Oncel E, Bicakcigil A,
Sancak B, Cengiz AB, Kara A, Ceyhan M: A comparison of blood stream
infections with extended spectrum beta-lactamase-producing and
non-producing Klebsiella pneumoniae in pediatric patients. Ital J
Pediatr 2017, 43(1):79. https://doi.org/10.1186/s13052-017-0398-0 PMid:28899399 PMCid:PMC5596860
- Arnan
M, Gudiol C, Calatayud L, Linares J, Dominguez MA, Batlle M, Ribera JM,
Carratala J, Gudiol F: Risk factors for, and clinical relevance of,
faecal extended-spectrum beta-lactamase producing Escherichia coli
(ESBL-EC) carriage in neutropenic patients with haematological
malignancies. Eur J Clin Microbiol Infect Dis 2011, 30(3):355-360. https://doi.org/10.1007/s10096-010-1093-x PMid:21052757
- Cornejo-Juarez
P, Suarez-Cuenca JA, Volkow-Fernandez P, Silva-Sanchez J,
Barrios-Camacho H, Najera-Leon E, Velazquez-Acosta C, Vilar-Compte D:
Fecal ESBL Escherichia coli carriage as a risk factor for bacteremia in
patients with hematological malignancies. Support Care Cancer 2016,
24(1):253-259. https://doi.org/10.1007/s00520-015-2772-z PMid:26014616
- Karthaus
M, Doellmann T, Klimasch T, Krauter J, Heil G, Ganser A: Central venous
catheter infections in patients with acute leukemia. Chemotherapy 2002,
48(3):154-157. https://doi.org/10.1159/000064922 PMid:12138333
- Theodoro
D, Olsen MA, Warren DK, McMullen KM, Asaro P, Henderson A, Tozier M,
Fraser V: Emergency Department Central Line-associated Bloodstream
Infections (CLABSI) Incidence in the Era of Prevention Practices. Acad
Emerg Med 2015, 22(9):1048-1055. https://doi.org/10.1111/acem.12744 PMid:26336036 PMCid:PMC4703118
- Kugler
E, Levi A, Goldberg E, Zaig E, Raanani P, Paul M: The association of
central venous catheter placement timing with infection rates in
patients with acute leukemia. Leuk Res 2015, 39(3):311-313. https://doi.org/10.1016/j.leukres.2014.12.017 PMid:25636357
- Jaeger
K, Zenz S, Juttner B, Ruschulte H, Kuse E, Heine J, Piepenbrock S,
Ganser A, Karthaus M: Reduction of catheter-related infections in
neutropenic patients: a prospective controlled randomized trial using a
chlorhexidine and silver sulfadiazine-impregnated central venous
catheter. Ann Hematol 2005, 84(4):258-262. https://doi.org/10.1007/s00277-004-0972-6 PMid:15549302
- Legrand
M, Max A, Peigne V, Mariotte E, Canet E, Debrumetz A, Lemiale V, Seguin
A, Darmon M, Schlemmer B et al: Survival in neutropenic patients with
severe sepsis or septic shock. Crit Care Med 2012, 40(1):43-49. https://doi.org/10.1097/CCM.0b013e31822b50c2 PMid:21926615
- Gao
Y, Liu Y, Ma X, Wei L, Chen W, Song L: The incidence and risk factors
of peripherally inserted central catheter-related infection among
cancer patients. Ther Clin Risk Manag 2015, 11:863-871. https://doi.org/10.2147/TCRM.S83776 PMid:26045668 PMCid:PMC4447175
- Singer
M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M,
Bellomo R, Bernard GR, Chiche JD, Coopersmith CM et al: The Third
International Consensus Definitions for Sepsis and Septic Shock
(Sepsis-3). JAMA 2016, 315(8):801-810. https://doi.org/10.1001/jama.2016.0287 PMid:26903338 PMCid:PMC4968574
- Ferreira
FL, Bota DP, Bross A, Melot C, Vincent JL: Serial evaluation of the
SOFA score to predict outcome in critically ill patients. Jama 2001,
286(14):1754-1758. https://doi.org/10.1001/jama.286.14.1754 PMid:11594901
- Bishop
JF, Matthews JP, Young GA, Szer J, Gillett A, Joshua D, Bradstock K,
Enno A, Wolf MM, Fox R et al: A randomized study of high-dose
cytarabine in induction in acute myeloid leukemia. Blood 1996,
87(5):1710-1717. https://doi.org/10.1182/blood.V87.5.1710.bloodjournal8751710 PMid:8634416
- Larson
RA, Dodge RK, Burns CP, Lee EJ, Stone RM, Schulman P, Duggan D, Davey
FR, Sobol RE, Frankel SR et al: A five-drug remission induction regimen
with intensive consolidation for adults with acute lymphoblastic
leukemia: cancer and leukemia group B study 8811. Blood 1995,
85(8):2025-2037. https://doi.org/10.1182/blood.V85.8.2025.bloodjournal8582025 PMid:7718875
- Levy
MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, Cohen J, Opal SM,
Vincent JL, Ramsay G et al: 2001 SCCM/ESICM/ACCP/ATS/SIS International
Sepsis Definitions Conference. Intensive Care Med 2003, 29(4):530-538. https://doi.org/10.1007/s00134-003-1662-x PMid:12664219
- Taplitz
RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, Langston AA,
Nastoupil LJ, Rajotte M, Rolston K et al: Outpatient Management of
Fever and Neutropenia in Adults Treated for Malignancy: American
Society of Clinical Oncology and Infectious Diseases Society of America
Clinical Practice Guideline Update. J Clin Oncol 2018,
36(14):1443-1453. https://doi.org/10.1200/JCO.2017.77.6211 PMid:29461916
- Klastersky
J, Paesmans M, Rubenstein EB, Boyer M, Elting L, Feld R, Gallagher J,
Herrstedt J, Rapoport B, Rolston K et al: The Multinational Association
for Supportive Care in Cancer risk index: A multinational scoring
system for identifying low-risk febrile neutropenic cancer patients. J
Clin Oncol 2000, 18(16):3038-3051. https://doi.org/10.1200/JCO.2000.18.16.3038 PMid:10944139
- Coyne
CJ, Le V, Brennan JJ, Castillo EM, Shatsky RA, Ferran K, Brodine S,
Vilke GM: Application of the MASCC and CISNE Risk-Stratification Scores
to Identify Low-Risk Febrile Neutropenic Patients in the Emergency
Department. Ann Emerg Med 2017, 69(6):755-764. https://doi.org/10.1016/j.annemergmed.2016.11.007 PMid:28041827
- Lee
SJ, Kim JH, Han SB, Paik JH, Durey A: Prognostic Factors Predicting
Poor Outcome in Cancer Patients with Febrile Neutropenia in the
Emergency Department: Usefulness of qSOFA. J Oncol 2018, 2018:2183179. https://doi.org/10.1155/2018/2183179 PMid:30405714 PMCid:PMC6201329
- Kim
M, Ahn S, Kim WY, Sohn CH, Seo DW, Lee YS, Lim KS: Predictive
performance of the quick score Sequential Organ Failure Assessment as a
screening tool for sepsis, mortality, and intensive care unit admission
in patients with febrile neutropenia. Support Care Cancer 2017,
25(5):1557-1562. https://doi.org/10.1007/s00520-016-3567-6 PMid:28062972
- Rolston
KV: Challenges in the treatment of infections caused by gram-positive
and gram-negative bacteria in patients with cancer and neutropenia.
Clin Infect Dis 2005, 40 Suppl 4:S246-252. https://doi.org/10.1086/427331 PMid:15768330
- Collin
BA, Leather HL, Wingard JR, Ramphal R: Evolution, incidence, and
susceptibility of bacterial bloodstream isolates from 519 bone marrow
transplant patients. Clin Infect Dis 2001, 33(7):947-953. https://doi.org/10.1086/322604 PMid:11528564
- Pittet
D, Tarara D, Wenzel RP: Nosocomial bloodstream infection in critically
ill patients. Excess length of stay, extra costs, and attributable
mortality. JAMA 1994, 271(20):1598-1601. https://doi.org/10.1001/jama.271.20.1598 PMid:8182812
- Klastersky
J: Current attitudes for therapy of febrile neutropenia with
consideration to cost-effectiveness. Curr Opin Oncol 1998,
10(4):284-290. https://doi.org/10.1097/00001622-199807000-00002 PMid:9702394
- Viscoli
C: The evolution of the empirical management of fever and neutropenia
in cancer patients. J Antimicrob Chemother 1998, 41 Suppl D:65-80. https://doi.org/10.1093/jac/41.suppl_4.65 PMid:9688453
- Armstrong D: History of opportunistic infection in the immunocompromised host. Clin Infect Dis 1993, 17 Suppl 2:S318-321. https://doi.org/10.1093/clinids/17.Supplement_2.S318 PMid:8274594
- Mayer
RJ, Davis RB, Schiffer CA, Berg DT, Powell BL, Schulman P, Omura GA,
Moore JO, McIntyre OR, Frei E, 3rd: Intensive postremission
chemotherapy in adults with acute myeloid leukemia. Cancer and Leukemia
Group B. N Engl J Med 1994, 331(14):896-903. https://doi.org/10.1056/NEJM199410063311402 PMid:8078551
- Lakshmaiah
KC, Malabagi AS, Govindbabu, Shetty R, Sinha M, Jayashree RS: Febrile
Neutropenia in Hematological Malignancies: Clinical and Microbiological
Profile and Outcome in High Risk Patients. J Lab Physicians 2015,
7(2):116-120. https://doi.org/10.4103/0974-2727.163126 PMid:26417163 PMCid:PMC4559624
- Freifeld
AG, Bow EJ, Sepkowitz KA, Boeckh MJ, Ito JI, Mullen CA, Raad, II,
Rolston KV, Young JA, Wingard JR et al: Clinical practice guideline for
the use of antimicrobial agents in neutropenic patients with cancer:
2010 update by the infectious diseases society of america. Clin Infect
Dis 2011, 52(4):e56-93. https://doi.org/10.1093/cid/cir073 PMid:21258094
- Dellinger
RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE,
Sprung CL, Douglas IS, Jaeschke R et al: Surviving sepsis campaign:
international guidelines for management of severe sepsis and septic
shock: 2012. Crit Care Med 2013, 41(2):580-637. https://doi.org/10.1007/s00134-012-2769-8 PMid:23361625
- Menzo
SL, la Martire G, Ceccarelli G, Venditti M: New Insight on Epidemiology
and Management of Bacterial Bloodstream Infection in Patients with
Hematological Malignancies. Mediterr J Hematol Infect Dis 2015,
7(1):e2015044. https://doi.org/10.4084/mjhid.2015.044 PMid:26185609 PMCid:PMC4500473
- Ricciardi
W, Giubbini G, Laurenti P: Surveillance and Control of Antibiotic
Resistance in the Mediterranean Region. Mediterr J Hematol Infect Dis
2016, 8(1):e2016036. https://doi.org/10.4084/mjhid.2016.036 PMid:27413528 PMCid:PMC4928537
- Bai
AD, Showler A, Burry L, Steinberg M, Ricciuto DR, Fernandes T, Chiu A,
Raybardhan S, Science M, Fernando E et al: Comparative effectiveness of
cefazolin versus cloxacillin as definitive antibiotic therapy for MSSA
bacteraemia: results from a large multicentre cohort study. J
Antimicrob Chemother 2015, 70(5):1539-1546. https://doi.org/10.1093/jac/dku560 PMid:25614044
- Hassoun
A, Linden PK, Friedman B: Incidence, prevalence, and management of MRSA
bacteremia across patient populations-a review of recent developments
in MRSA management and treatment. Crit Care 2017, 21(1):211. https://doi.org/10.1186/s13054-017-1801-3 PMid:28807042 PMCid:PMC5557425
- Mikulska
M, Del Bono V, Viscoli C: Bacterial infections in hematopoietic stem
cell transplantation recipients. Curr Opin Hematol 2014, 21(6):451-458.
https://doi.org/10.1097/MOH.0000000000000088 PMid:25295742
- Satlin
MJ, Walsh TJ: Multidrug-resistant Enterobacteriaceae, Pseudomonas
aeruginosa, and vancomycin-resistant Enterococcus: Three major threats
to hematopoietic stem cell transplant recipients. Transpl Infect Dis
2017, 19(6). https://doi.org/10.1111/tid.12762 PMid:28815897 PMCid:PMC5745272
- Bartlett
JG: Narrative review: the new epidemic of Clostridium
difficile-associated enteric disease. Annals of internal medicine 2006,
145(10):758-764. https://doi.org/10.7326/0003-4819-145-10-200611210-00008 PMid:17116920
- Torfoss D: Carbapenems and febrile neutropenia - author's reply. Clin Microbiol Infect 2017, 23(3):214. https://doi.org/10.1016/j.cmi.2016.12.019 PMid:28025133
- Torfoss
D, Fladhagen T, Holte H, Brinch L, Schjesvold FH, Floisand Y, Nyquist
E, Dalgaard J, Meyer P, Lehmann AK et al: Benzylpenicillin plus an
aminoglycoside versus meropenem in neutropenic lymphoma and leukaemia
patients with a suspected bacterial infection: a randomized, controlled
trial. Clin Microbiol Infect 2017, 23(3):179-187. https://doi.org/10.1016/j.cmi.2016.10.019 PMid:27793737
- Torfoss
D, Hoiby EA, Holte H, Kvaloy S: The Norwegian experience with
penicillin G plus an aminoglycoside as initial empiric therapy in
febrile neutropenia; a review. Acta Oncol 2012, 51(4):433-440. https://doi.org/10.3109/0284186X.2011.633931 PMid:22175253
- Torfoss
D, Hoiby EA, Tangen JM, Holte H, Bo K, Meyer P, Grottum K, Weyde K,
Lauritzsen GF, Sandstad B et al: Tobramycin once versus three times
daily, given with penicillin G, to febrile neutropenic cancer patients
in Norway: a prospective, randomized, multicentre trial. J Antimicrob
Chemother 2007, 59(4):711-717.https://doi.org/10.1093/jac/dkm003 PMid:17327294
- Perez
F, Adachi J, Bonomo RA: Antibiotic-resistant gram-negative bacterial
infections in patients with cancer. Clin Infect Dis 2014, 59 Suppl
5:S335-339. https://doi.org/10.1093/cid/ciu612 PMid:25352627 PMCid:PMC4303050
- Gudiol
C, Royo-Cebrecos C, Tebe C, Abdala E, Akova M, Alvarez R, Maestro-de la
Calle G, Cano A, Cervera C, Clemente WT et al: Clinical efficacy of
beta-lactam/beta-lactamase inhibitor combinations for the treatment of
bloodstream infection due to extended-spectrum beta-lactamase-producing
Enterobacteriaceae in haematological patients with neutropaenia: a
study protocol for a retrospective observational study (BICAR). BMJ
Open 2017, 7(1):e013268. https://doi.org/10.1136/bmjopen-2016-013268 PMid:28115333 PMCid:PMC5278288
- Bassetti
M, Giacobbe DR, Giamarellou H, Viscoli C, Daikos GL, Dimopoulos G, De
Rosa FG, Giamarellos-Bourboulis EJ, Rossolini GM, Righi E et al:
Management of KPC-producing Klebsiella pneumoniae infections. Clin
Microbiol Infect 2018, 24(2):133-144. https://doi.org/10.1016/j.cmi.2017.08.030 PMid:28893689
- Gutierrez-Gutierrez
B, Salamanca E, de Cueto M, Hsueh PR, Viale P, Pano-Pardo JR, Venditti
M, Tumbarello M, Daikos G, Canton R et al: Effect of appropriate
combination therapy on mortality of patients with bloodstream
infections due to carbapenemase-producing Enterobacteriaceae
(INCREMENT): a retrospective cohort study. Lancet Infect Dis 2017,
17(7):726-734.
- Gutierrez-Gutierrez B,
Perez-Galera S, Salamanca E, de Cueto M, Calbo E, Almirante B, Viale P,
Oliver A, Pintado V, Gasch O et al: A Multinational, Preregistered
Cohort Study of beta-Lactam/beta-Lactamase Inhibitor Combinations for
Treatment of Bloodstream Infections Due to
Extended-Spectrum-beta-Lactamase-Producing Enterobacteriaceae.
Antimicrob Agents Chemother 2016, 60(7):4159-4169. https://doi.org/10.1128/AAC.00365-16 PMid:27139473 PMCid:PMC4914653
- Averbuch
D, Cordonnier C, Livermore DM, Mikulska M, Orasch C, Viscoli C, Gyssens
IC, Kern WV, Klyasova G, Marchetti O et al: Targeted therapy against
multi-resistant bacteria in leukemic and hematopoietic stem cell
transplant recipients: guidelines of the 4th European Conference on
Infections in Leukemia (ECIL-4, 2011). Haematologica 2013,
98(12):1836-1847. https://doi.org/10.3324/haematol.2013.091330 PMid:24323984 PMCid:PMC3856958
- Kengkla
K, Kongpakwattana K, Saokaew S, Apisarnthanarak A, Chaiyakunapruk N:
Comparative efficacy and safety of treatment options for MDR and XDR
Acinetobacter baumannii infections: a systematic review and network
meta-analysis. J Antimicrob Chemother 2018, 73(1):22-32. https://doi.org/10.1093/jac/dkx368 PMid:29069421
- Averbuch
D, Tridello G, Hoek J, Mikulska M, Akan H, Yanez San Segundo L, Pabst
T, Ozcelik T, Klyasova G, Donnini I et al: Antimicrobial Resistance in
Gram-Negative Rods Causing Bacteremia in Hematopoietic Stem Cell
Transplant Recipients: Intercontinental Prospective Study of the
Infectious Diseases Working Party of the European Bone Marrow
Transplantation Group. Clin Infect Dis 2017, 65(11):1819-1828. https://doi.org/10.1093/cid/cix646 PMid:29020364
- Mikulska
M, Averbuch D, Tissot F, Cordonnier C, Akova M, Calandra T, Ceppi M,
Bruzzi P, Viscoli C, European Conference on Infections in L:
Fluoroquinolone prophylaxis in haematological cancer patients with
neutropenia: ECIL critical appraisal of previous guidelines. J Infect
2018, 76(1):20-37. https://doi.org/10.1016/j.jinf.2017.10.009 PMid:29079323
- Karimi
F, Ashrafi F, Moghaddas A, Derakhshandeh A: Management of Febrile
Neutropenia: A Description of Clinical and Microbiological Findings by
Focusing on Risk Factors and Pitfalls. J Res Pharm Pract 2018,
7(3):147-156. https://doi.org/10.4103/jrpp.JRPP_18_16 PMid:30211240 PMCid:PMC6121758
- Gustinetti
G, Mikulska M: Bloodstream infections in neutropenic cancer patients: A
practical update. Virulence 2016, 7(3):280-297. https://doi.org/10.1080/21505594.2016.1156821 PMid:27002635 PMCid:PMC4871679
- Wisplinghoff
H, Seifert H, Wenzel RP, Edmond MB: Current trends in the epidemiology
of nosocomial bloodstream infections in patients with hematological
malignancies and solid neoplasms in hospitals in the United States.
Clin Infect Dis 2003, 36(9):1103-1110. https://doi.org/10.1086/374339 PMid:12715303
- van
Duin D, Paterson DL: Multidrug-Resistant Bacteria in the Community:
Trends and Lessons Learned. Infect Dis Clin North Am 2016,
30(2):377-390. https://doi.org/10.1016/j.idc.2016.02.004 PMid:27208764 PMCid:PMC5314345
- Laws
M, Shaaban A, Rahman KM: Antibiotic resistance breakers: current
approaches and future directions. FEMS Microbiol Rev 2019,
43(5):490-516. https://doi.org/10.1093/femsre/fuz014 PMid:31150547 89:PMC6736374
- Averbuch
D, Orasch C, Cordonnier C, Livermore DM, Mikulska M, Viscoli C, Gyssens
IC, Kern WV, Klyasova G, Marchetti O et al: European guidelines for
empirical antibacterial therapy for febrile neutropenic patients in the
era of growing resistance: summary of the 2011 4th European Conference
on Infections in Leukemia. Haematologica 2013, 98(12):1826-1835. https://doi.org/10.3324/haematol.2013.091025 PMid:24323983 PMCid:PMC3856957
- Balletto
E, Mikulska M: Bacterial Infections in Hematopoietic Stem Cell
Transplant Recipients. Mediterr J Hematol Infect Dis 2015,
7(1):e2015045. https://doi.org/10.4084/mjhid.2015.045 PMid:26185610 PMCid:PMC4500472
- Mikulska
M, Viscoli C, Orasch C, Livermore DM, Averbuch D, Cordonnier C, Akova
M, Fourth European Conference on Infections in Leukemia Group
ajvoEEIELN, Esgich/Escmid: Aetiology and resistance in bacteraemias
among adult and paediatric haematology and cancer patients. J Infect
2014, 68(4):321-331. https://doi.org/10.1016/j.jinf.2013.12.006 PMid:24370562
- Lambert PA: Mechanisms of antibiotic resistance in Pseudomonas aeruginosa. J R Soc Med 2002, 95 Suppl 41:22-26.
- Horasan
ES, Ersoz G, Tombak A, Tiftik N, Kaya A: Bloodstream infections and
mortality-related factors in febrile neutropenic cancer patients. Med
Sci Monit 2011, 17(5):CR304-309. https://doi.org/10.12659/MSM.881773 PMid:21525814 PMCid:PMC3539578
- Kolonen
A, Sinisalo M, Huttunen R, Syrjanen J, Aittoniemi J, Huhtala H, Sankelo
M, Rintala H, Raty R, Jantunen E et al: Bloodstream infections in acute
myeloid leukemia patients treated according to the Finnish Leukemia
Group AML-2003 protocol - a prospective nationwide study. Infect Dis
(Lond) 2017, 49(11-12):799-808. https://doi.org/10.1080/23744235.2017.1347814 PMid:28683646
- Macesic
N, Morrissey CO, Cheng AC, Spencer A, Peleg AY: Changing microbial
epidemiology in hematopoietic stem cell transplant recipients:
increasing resistance over a 9-year period. Transpl Infect Dis 2014,
16(6):887-896. https://doi.org/10.1111/tid.12298 PMid:25298044
- Vydra
J, Shanley RM, George I, Ustun C, Smith AR, Weisdorf DJ, Young JA:
Enterococcal bacteremia is associated with increased risk of mortality
in recipients of allogeneic hematopoietic stem cell transplantation.
Clin Infect Dis 2012, 55(6):764-770. https://doi.org/10.1093/cid/cis550 PMid:22693346 PMCid:PMC3657510
- Tavadze
M, Rybicki L, Mossad S, Avery R, Yurch M, Pohlman B, Duong H, Dean R,
Hill B, Andresen S et al: Risk factors for vancomycin-resistant
enterococcus bacteremia and its influence on survival after allogeneic
hematopoietic cell transplantation. Bone Marrow Transplant 2014,
49(10):1310-1316. https://doi.org/10.1038/bmt.2014.150 PMid:25111516
- Jaffe
D, Jakubowski A, Sepkowitz K, Sebti R, Kiehn TE, Pamer E, Papanicolaou
GA: Prevention of peritransplantation viridans streptococcal bacteremia
with early vancomycin administration: a single-center observational
cohort study. Clin Infect Dis 2004, 39(11):1625-1632. https://doi.org/10.1086/425612 PMid:15578362
- Shenep JL: Viridans-group streptococcal infections in immunocompromised hosts. Int J Antimicrob Agents 2000, 14(2):129-135. https://doi.org/10.1016/S0924-8579(99)00172-7
- Freifeld
A, Marchigiani D, Walsh T, Chanock S, Lewis L, Hiemenz J, Hiemenz S,
Hicks JE, Gill V, Steinberg SM et al: A double-blind comparison of
empirical oral and intravenous antibiotic therapy for low-risk febrile
patients with neutropenia during cancer chemotherapy. N Engl J Med
1999, 341(5):305-311. https://doi.org/10.1056/NEJM199907293410501 PMid:10423464
- Lodise
TP, Jr., Lomaestro B, Drusano GL: Piperacillin-tazobactam for
Pseudomonas aeruginosa infection: clinical implications of an
extended-infusion dosing strategy. Clin Infect Dis 2007, 44(3):357-363.
https://doi.org/10.1086/510590 PMid:17205441
- Krause KM, Serio AW, Kane TR, Connolly LE: Aminoglycosides: An Overview. Cold Spring Harb Perspect Med 2016, 6(6). https://doi.org/10.1101/cshperspect.a027029 PMid:27252397 PMCid:PMC4888811
- Kassamali
Z, Danziger L: To B or not to B, that is the question: is it time to
replace colistin with polymyxin B? Pharmacotherapy 2015, 35(1):17-21. https://doi.org/10.1002/phar.1510 PMid:25346395
- Parker
S, Lipman J, Koulenti D, Dimopoulos G, Roberts JA: What is the
relevance of fosfomycin pharmacokinetics in the treatment of serious
infections in critically ill patients? A systematic review. Int J
Antimicrob Agents 2013, 42(4):289-293. https://doi.org/10.1016/j.ijantimicag.2013.05.018 PMid:23880170
- Maschmeyer
G, Helweg-Larsen J, Pagano L, Robin C, Cordonnier C, Schellongowski P:
ECIL guidelines for treatment of Pneumocystis jirovecii pneumonia in
non-HIV-infected haematology patients. J Antimicrob Chemother 2016,
71(9):2405-2413. https://doi.org/10.1093/jac/dkw158 PMid:27550993
- Gums
JG, Boatwright DW, Camblin M, Halstead DC, Jones ME, Sanderson R:
Differences between ceftriaxone and cefotaxime: microbiological
inconsistencies. Ann Pharmacother 2008, 42(1):71-79. https://doi.org/10.1345/aph.1H620 PMid:18094350
- Bijie
H, Kulpradist S, Manalaysay M, Soebandrio A: In vitro activity,
pharmacokinetics, clinical efficacy, safety and pharmacoeconomics of
ceftriaxone compared with third and fourth generation cephalosporins:
review. J Chemother 2005, 17(1):3-24.
- Wang
FD, Liu CY, Hsu HC, Gau JP, Chau WK, Haung ML, Ho CH: A comparative
study of cefepime versus ceftazidime as empiric therapy of febrile
episodes in neutropenic patients. Chemotherapy 1999, 45(5):370-379. https://doi.org/10.1159/000007228 PMid:10473925
- Seymour
CW, Gesten F, Prescott HC, Friedrich ME, Iwashyna TJ, Phillips GS,
Lemeshow S, Osborn T, Terry KM, Levy MM: Time to Treatment and
Mortality during Mandated Emergency Care for Sepsis. N Engl J Med 2017,
376(23):2235-2244. https://doi.org/10.1056/NEJMoa1703058 PMid:28528569 PMCid:PMC5538258
- Wendelbo
O, Hervig T, Haugen O, Seghatchian J, Reikvam H: Microcirculation and
red cell transfusion in patients with sepsis. Transfus Apher Sci 2017,
56(6):900-905. https://doi.org/10.1016/j.transci.2017.11.020 PMid:29158076
- Klastersky J: Empirical antibiotic therapy in neutropenic cancer patients. Eur J Cancer 1993, 29A Suppl 1:S6-10. https://doi.org/10.1016/S0959-8049(05)80253-9
- Groll
AH, Castagnola E, Cesaro S, Dalle JH, Engelhard D, Hope W, Roilides E,
Styczynski J, Warris A, Lehrnbecher T: Fourth European Conference on
Infections in Leukaemia (ECIL-4): guidelines for diagnosis, prevention,
and treatment of invasive fungal diseases in paediatric patients with
cancer or allogeneic haemopoietic stem-cell transplantation. Lancet
Oncol 2014, 15(8):e327-340. https://doi.org/10.1016/S1470-2045(14)70017-8
- Gudiol
C, Royo-Cebrecos C, Abdala E, Akova M, Alvarez R, Maestro-de la Calle
G, Cano A, Cervera C, Clemente WT, Martin-Davila P et al: Efficacy of
beta-Lactam/beta-Lactamase Inhibitor Combinations for the Treatment of
Bloodstream Infection Due to Extended-Spectrum-beta-Lactamase-Producing
Enterobacteriaceae in Hematological Patients with Neutropenia.
Antimicrob Agents Chemother 2017, 61(8). https://doi.org/10.1128/AAC.00164-17 PMid:28584145 PMCid:PMC5527609
- Adegoke
AA, Stenstrom TA, Okoh AI: Stenotrophomonas maltophilia as an Emerging
Ubiquitous Pathogen: Looking Beyond Contemporary Antibiotic Therapy.
Front Microbiol 2017, 8:2276. https://doi.org/10.3389/fmicb.2017.02276 PMid:29250041 PMCid:PMC5714879
- Vardakas
KZ, Tansarli GS, Bliziotis IA, Falagas ME: beta-Lactam plus
aminoglycoside or fluoroquinolone combination versus beta-lactam
monotherapy for Pseudomonas aeruginosa infections: a meta-analysis. Int
J Antimicrob Agents 2013, 41(4):301-310. https://doi.org/10.1016/j.ijantimicag.2012.12.006 PMid:23410791
- Davies J, Davies D: Origins and evolution of antibiotic resistance. Microbiol Mol Biol Rev 2010, 74(3):417-433. https://doi.org/10.1128/MMBR.00016-10 PMid:20805405 PMCid:PMC2937522
- Hammond
SP, Marty FM, Bryar JM, DeAngelo DJ, Baden LR: Invasive fungal disease
in patients treated for newly diagnosed acute leukemia. Am J Hematol
2010, 85(9):695-699. https://doi.org/10.1002/ajh.21776 PMid:20652970
- Auberger
J, Lass-Florl C, Ulmer H, Nogler-Semenitz E, Clausen J, Gunsilius E,
Einsele H, Gastl G, Nachbaur D: Significant alterations in the
epidemiology and treatment outcome of invasive fungal infections in
patients with hematological malignancies. Int J Hematol 2008,
88(5):508-515. https://doi.org/10.1007/s12185-008-0184-2 PMid:18982251
- Ullmann
AJ, Akova M, Herbrecht R, Viscoli C, Arendrup MC, Arikan-Akdagli S,
Bassetti M, Bille J, Calandra T, Castagnola E et al: ESCMID* guideline
for the diagnosis and management of Candida diseases 2012: adults with
haematological malignancies and after haematopoietic stem cell
transplantation (HCT). Clin Microbiol Infect 2012, 18 Suppl 7:53-67. https://doi.org/10.1111/1469-0691.12041 PMid:23137137
- Chamilos
G, Luna M, Lewis RE, Bodey GP, Chemaly R, Tarrand JJ, Safdar A, Raad,
II, Kontoyiannis DP: Invasive fungal infections in patients with
hematologic malignancies in a tertiary care cancer center: an autopsy
study over a 15-year period (1989-2003). Haematologica 2006,
91(7):986-989.
- Pagano L, Caira M,
Candoni A, Offidani M, Fianchi L, Martino B, Pastore D, Picardi M,
Bonini A, Chierichini A et al: The epidemiology of fungal infections in
patients with hematologic malignancies: the SEIFEM-2004 study.
Haematologica 2006, 91(8):1068-1075.
- Ananda-Rajah
MR, Grigg A, Downey MT, Bajel A, Spelman T, Cheng A, Thursky KT,
Vincent J, Slavin MA: Comparative clinical effectiveness of
prophylactic voriconazole/posaconazole to fluconazole/itraconazole in
patients with acute myeloid leukemia/myelodysplastic syndrome
undergoing cytotoxic chemotherapy over a 12-year period. Haematologica
2012, 97(3):459-463. https://doi.org/10.3324/haematol.2011.051995 PMid:22058198 PMCid:PMC329160
- Sipsas
NV, Lewis RE, Tarrand J, Hachem R, Rolston KV, Raad, II, Kontoyiannis
DP: Candidemia in patients with hematologic malignancies in the era of
new antifungal agents (2001-2007): stable incidence but changing
epidemiology of a still frequently lethal infection. Cancer 2009,
115(20):4745-4752. https://doi.org/10.1002/cncr.24507 PMid:19634156
- von
Lilienfeld-Toal M, Wagener J, Einsele H, Cornely OA, Kurzai O: Invasive
Fungal Infection. Dtsch Arztebl Int 2019, 116(16):271-278. https://doi.org/10.3238/arztebl.2019.0271 PMid:31159914 PMCid:PMC6549129
- Maini
R, Henderson KL, Sheridan EA, Lamagni T, Nichols G, Delpech V, Phin N:
Increasing Pneumocystis pneumonia, England, UK, 2000-2010. Emerg Infect
Dis 2013, 19(3):386-392. https://doi.org/10.3201/eid1903.121151 PMid:23622345 PMCid:PMC3647665
- Rajasingham
R, Smith RM, Park BJ, Jarvis JN, Govender NP, Chiller TM, Denning DW,
Loyse A, Boulware DR: Global burden of disease of HIV-associated
cryptococcal meningitis: an updated analysis. Lancet Infect Dis 2017,
17(8):873-881. https://doi.org/10.1016/S1473-3099(17)30243-8
- Prakash H, Chakrabarti A: Global Epidemiology of Mucormycosis. J Fungi (Basel) 2019, 5(1). https://doi.org/10.3390/jof5010026 PMid:30901907 PMCid:PMC6462913
- Seitz
AE, Adjemian J, Steiner CA, Prevots DR: Spatial epidemiology of
blastomycosis hospitalizations: detecting clusters and identifying
environmental risk factors. Med Mycol 2015, 53(5):447-454. https://doi.org/10.1093/mmy/myv014 PMid:25908653
- Keighley
C, Chen SC, Marriott D, Pope A, Chapman B, Kennedy K, Bak N, Underwood
N, Wilson HL, McDonald K et al: Candidaemia and a risk predictive model
for overall mortality: a prospective multicentre study. BMC Infect Dis
2019, 19(1):445. https://doi.org/10.1186/s12879-019-4065-5 PMid:31113382 PMCid:PMC6528341
- Pagano
L, Antinori A, Ammassari A, Mele L, Nosari A, Melillo L, Martino B,
Sanguinetti M, Equitani F, Nobile F et al: Retrospective study of
candidemia in patients with hematological malignancies. Clinical
features, risk factors and outcome of 76 episodes. Eur J Haematol 1999,
63(2):77-85. https://doi.org/10.1111/j.1600-0609.1999.tb01120.x PMid:10480286
- Horn
DL, Neofytos D, Anaissie EJ, Fishman JA, Steinbach WJ, Olyaei AJ, Marr
KA, Pfaller MA, Chang CH, Webster KM: Epidemiology and outcomes of
candidemia in 2019 patients: data from the prospective antifungal
therapy alliance registry. Clin Infect Dis 2009, 48(12):1695-1703. https://doi.org/10.1086/599039 PMid:19441981
- Wisplinghoff
H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, Edmond MB: Nosocomial
bloodstream infections in US hospitals: analysis of 24,179 cases from a
prospective nationwide surveillance study. Clin Infect Dis 2004,
39(3):309-317. https://doi.org/10.1086/421946 PMid:15306996
- Nicolle
MC, Benet T, Thiebaut A, Bienvenu AL, Voirin N, Duclos A, Sobh M,
Cannas G, Thomas X, Nicolini FE et al: Invasive aspergillosis in
patients with hematologic malignancies: incidence and description of
127 cases enrolled in a single institution prospective survey from 2004
to 2009. Haematologica 2011, 96(11):1685-1691. https://doi.org/10.3324/haematol.2011.044636 PMid:21791468 PMCid:PMC3208687
- Bhatt VR, Viola GM, Ferrajoli A: Invasive fungal infections in acute leukemia. Ther Adv Hematol 2011, 2(4):231-247. https://doi.org/10.1177/2040620711410098 PMid:23556092 PMCid:PMC3573411
- Lone SA, Ahmad A: Candida auris-the growing menace to global health. Mycoses 2019, 62(8):620-637. https://doi.org/10.1111/myc.12904 PMid:30773703
- Patel
HP, Perissinotti AJ, Patel TS, Bixby DL, Marshall VD, Marini BL:
Incidence and Risk Factors for Breakthrough Invasive Mold Infections in
Acute Myeloid Leukemia Patients Receiving Remission Induction
Chemotherapy. Open Forum Infect Dis 2019, 6(5):ofz176. https://doi.org/10.1093/ofid/ofz176 PMid:31123689 PMCid:PMC6524834
- Kimura
M, Araoka H, Yamamoto H, Asano-Mori Y, Nakamura S, Yamagoe S, Ohno H,
Miyazaki Y, Abe M, Yuasa M et al: Clinical and Microbiological
Characteristics of Breakthrough Candidemia in Allogeneic Hematopoietic
Stem Cell Transplant Recipients in a Japanese Hospital. Antimicrob
Agents Chemother 2017, 61(4). https://doi.org/10.1128/AAC.01791-16 PMid:28115352 PMCid:PMC5365651
- Mercier
T, Maertens J: Clinical considerations in the early treatment of
invasive mould infections and disease. J Antimicrob Chemother 2017,
72(suppl_1):i29-i38. https://doi.org/10.1093/jac/dkx031 PMid:28355465
- Tissot
F, Agrawal S, Pagano L, Petrikkos G, Groll AH, Skiada A, Lass-Florl C,
Calandra T, Viscoli C, Herbrecht R: ECIL-6 guidelines for the treatment
of invasive candidiasis, aspergillosis and mucormycosis in leukemia and
hematopoietic stem cell transplant patients. Haematologica 2017,
102(3):433-444. https://doi.org/10.3324/haematol.2016.152900 PMid:28011902 PMCid:PMC5394968
- Andes
DR, Safdar N, Baddley JW, Playford G, Reboli AC, Rex JH, Sobel JD,
Pappas PG, Kullberg BJ: Impact of treatment strategy on outcomes in
patients with candidemia and other forms of invasive candidiasis: a
patient-level quantitative review of randomized trials. Clin Infect Dis
2012, 54(8):1110-1122. https://doi.org/10.1093/cid/cis021 PMid:22412055
- Maertens
JA, Raad, II, Marr KA, Patterson TF, Kontoyiannis DP, Cornely OA, Bow
EJ, Rahav G, Neofytos D, Aoun M et al: Isavuconazole versus
voriconazole for primary treatment of invasive mould disease caused by
Aspergillus and other filamentous fungi (SECURE): a phase 3,
randomised-controlled, non-inferiority trial. Lancet 2016,
387(10020):760-769. https://doi.org/10.1016/S0140-6736(15)01159-9
- Skiada
A, Lanternier F, Groll AH, Pagano L, Zimmerli S, Herbrecht R,
Lortholary O, Petrikkos GL, European Conference on Infections in L:
Diagnosis and treatment of mucormycosis in patients with hematological
malignancies: guidelines from the 3rd European Conference on Infections
in Leukemia (ECIL 3). Haematologica 2013, 98(4):492-504. https://doi.org/10.3324/haematol.2012.065110 PMid:22983580 PMCid:PMC3659979
- Walsh
TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA,
Morrison VA, Segal BH, Steinbach WJ, Stevens DA et al: Treatment of
aspergillosis: clinical practice guidelines of the Infectious Diseases
Society of America. Clin Infect Dis 2008, 46(3):327-360. https://doi.org/10.1086/525258 PMid:18177225
- Gafter-Gvili
A, Fraser A, Paul M, Vidal L, Lawrie TA, van de Wetering MD, Kremer LC,
Leibovici L: Antibiotic prophylaxis for bacterial infections in
afebrile neutropenic patients following chemotherapy. Cochrane Database
Syst Rev 2012, 1:CD004386. https://doi.org/10.1002/14651858.CD004386.pub3 PMCid:PMC4170789
- Paterson
DL, Mulazimoglu L, Casellas JM, Ko WC, Goossens H, Von Gottberg A,
Mohapatra S, Trenholme GM, Klugman KP, McCormack JG et al: Epidemiology
of ciprofloxacin resistance and its relationship to extended-spectrum
beta-lactamase production in Klebsiella pneumoniae isolates causing
bacteremia. Clin Infect Dis 2000, 30(3):473-478. https://doi.org/10.1086/313719 PMid:10722430
- Slavin
MA, Lingaratnam S, Mileshkin L, Booth DL, Cain MJ, Ritchie DS, Wei A,
Thursky KA, Australian Consensus Guidelines Steering C: Use of
antibacterial prophylaxis for patients with neutropenia. Australian
Consensus Guidelines 2011 Steering Committee. Intern Med J 2011,
41(1b):102-109. https://doi.org/10.1111/j.1445-5994.2010.02341.x PMid:21272174
- Taplitz
RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, Langston AA,
Nastoupil LJ, Rajotte M, Rolston KV et al: Antimicrobial Prophylaxis
for Adult Patients With Cancer-Related Immunosuppression: ASCO and IDSA
Clinical Practice Guideline Update. J Clin Oncol 2018,
36(30):3043-3054. https://doi.org/10.1200/JCO.18.00374 PMid:30179565
- Maertens
JA, Girmenia C, Bruggemann RJ, Duarte RF, Kibbler CC, Ljungman P, Racil
Z, Ribaud P, Slavin MA, Cornely OA et al: European guidelines for
primary antifungal prophylaxis in adult haematology patients: summary
of the updated recommendations from the European Conference on
Infections in Leukaemia. J Antimicrob Chemother 2018, 73(12):3221-3230.
https://doi.org/10.1093/jac/dky286
- Patel RA, Gallagher JC: Drug fever. Pharmacotherapy 2010, 30(1):57-69. https://doi.org/10.1592/phco.30.1.57 PMid:20030474
- Toussaint
E, Bahel-Ball E, Vekemans M, Georgala A, Al-Hakak L, Paesmans M, Aoun
M: Causes of fever in cancer patients (prospective study over 477
episodes). Support Care Cancer 2006, 14(7):763-769. https://doi.org/10.1007/s00520-005-0898-0 PMid:16528534
- Mosevoll
KA, Johansen S, Wendelbo O, Nepstad I, Bruserud O, Reikvam H:
Cytokines, Adhesion Molecules, and Matrix Metalloproteases as
Predisposing, Diagnostic, and Prognostic Factors in Venous Thrombosis.
Front Med (Lausanne) 2018, 5:147. https://doi.org/10.3389/fmed.2018.00147 PMid:29872658 PMCid:PMC5972295
- Racanelli
V, Prete M, Minoia C, Favoino E, Perosa F: Rheumatic disorders as
paraneoplastic syndromes. Autoimmun Rev 2008, 7(5):352-358. https://doi.org/10.1016/j.autrev.2008.02.001 PMid:18486921
[TOP]