Received: November 25, 2013
Accepted: December 2, 2013
Meditter J Hematol Infect Dis 2014, 6(1): e2014007, DOI 10.4084/MJHID.2014.007
This article is available on PDF format at:

Tomasz Sacha
Department of Hematology,
Collegium Medicum, Jagiellonian University, Cracow, Poland.
|
This
is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract Imatinib was the
first signal transduction inhibitor (STI), used in a clinical setting.
It prevents a BCR-ABL protein from exerting its role in the oncogenic
pathway in chronic myeloid leukemia (CML). Imatinib directly inhibits
the constitutive tyrosine kinase activity. Imatinib binds to BCR-ABL
kinase domain by preventing the transfer of a phosphate group to
tyrosine on the protein substrate and the subsequent activation of
phosphorylated protein. As the result, the transmission of
proliferative signals to the nucleus is blocked and leukemic cell
apoptosis is induced. The FDA has approved imatinib as first-line
treatment for newly diagnosed CML in December 2002 following an
International Randomized Study (IRIS), initiated in June 2000,
comparing imatinib at a single daily dose 400 mg to IFN alpha plus
cytarabine in newly diagnosed patients with CML in CP. Results from
this study show the outstanding effectiveness of imatinib and its
superiority with respect to the rates of complete hematological
response (CHR), major and complete cytogenetic response (MCyR, CCyR).
Patients randomized to imatinib arm at 8 – year data cut off continue
to have a durable hematologic and cytogenetic response, low progression
rates to AP or BC, and remarkable survival outcomes. An overall
survival (OS) rate is 85% for patients receiving imatinib (93% when
only CML-related deaths and those prior to stem cell transplantation
are considered). The results have been confirmed in the last years by
several groups. According these cumulative results the rates of CCyR
achieved after one year of therapy with imatinib at standard dose
ranged from 49% to 77%, and the proportion of patients who achieved
major molecular response (MMR) after one year ranged between 18% and
58%. Discontinuation of imatinib has been also tried in patients in
MMR, a molecular relapse occurs in about one third of patients,
generally within 6 months from imatinib cessation.
|
Introduction
Imatinib
was the first signal transduction inhibitor (STI), used in a clinical
setting. It prevents a BCR-ABL protein from exerting its role in the
oncogenic pathway in chronic myeloid leukemia (CML). Imatinib directly
inhibits the constitutive tyrosine kinase activity, which results in
the modification of the function of various genes involved in the
control of the cell cycle, cell adhesion, cytoskeleton organization and
finally in the apoptotic death of Ph(+) cells.[1]
Imatinib binds to BCR-ABL kinase domain, which is in an inactive
conformation in a pocket reserved for the ATP binding site, thus
preventing the transfer of a phosphate group to tyrosine on the protein
substrate and the subsequent activation of phosphorylated protein. As
the result, the transmission of proliferative signals to the nucleus is
blocked and leukemic cell apoptosis is induced.[2]
Preclinical in vitro
studies showed that imatinib is a tyrosine kinase inhibitor (TKI) of
ABL kinase and its active derivatives: viral Abelson nonreceptor
protein tyrosine kinase (v-ABL), BCR-ABL,[3,4]
TEL-ABL,[5]
platelet-derived growth factor receptor (PDGFR) and Steel factor
receptor (c-KIT) kinases.[6]
Imatinib exhibits high level of
selectivity. Its activity against the above protein kinases is similar
with IC50 values in the range of 0.025 M for protein
autophosphorylation and is at least 100-fold lower than for a large
number of other tyrosine and serine/threonine kinases.[6]
Pharmacokinetics of Imatinib
Pharmacokinetics of imatinib is characterized by rapid and complete
oral bioavailability (98%) and a proportional dose-exposure
relationship.[18,19] There is no
significant interaction of imatinib
with food intake. Its terminal half-life is approximately 18 hours,
allowing for once-daily dosing.[18,19]
The median peak plasma
concentrations at steady state of imatinib administered orally once a
day at a dose of 400 mg and median trough levels are 5.4 M, and 1.43 M
respectively.[7] Imatinib is
metabolized by the cytochrome P450 system.
CYP3A4 is the major isoenzyme responsible for imatinib metabolism,
although CYP1A2, CYP2D6, CYP2C9, and CYP2C19 also contribute to a minor
extent.[18,19] The activity of CYP
enzyme exhibits intrinsic
variability, which could be the cause of high interpatient unevenness
in imatinib exposure.[18,19] Drugs
that are inhibitors or inductors of
the CYP3A4 isoenzyme have been shown to alter imatinib pharmacokinetic
activity.[20]
Efficacy of Imatinib
Phase
I trials:
The first phase I trial was initiated in June 1998 and enrolled
patients suffering from CML in chronic phase (CP) who were resistant to
or intolerant of interferon alpha (IFN alpha). Almost all patients
(98%) treated with at least 300 mg imatinib per day achieved complete
hematological response (CHR). Major and complete cytogenetic response
(MCyR, CCyR) were obtained by 31% and 13% of patients respectively. Of
note, the responses were durable, only 2 relapses (out of 53
patients) were noted after a median follow-up of 265 days.[8] Based on
these results, the protocol was expanded and included 58 patients in
blast crisis (BC) or with Ph-positive acute lymphoblastic leukemia
(Ph+ALL). Hematological responses to minimal dose of imatinib in this
cohort (300 mg daily) were obtained in 55% and 70% of patients with
myeloid, and lymphoid blast crisis respectively, including four CHR in
each group. Twelve percent of patients achieved MCyR and 8% CCyR.
Patients treated in BC unlike patients treated in the CP relapsed
frequently after initiating imatinib therapy. Approximately 50% of
responders with myeloid phenotype and all but one responder with
lymphoid phenotype relapsed between 42 and 193 days of imatinib
treatment (Druker et al., 2001b). Patients in accelerated phase (AP)
had not been studied in the phase I protocols.
Phase
II trials:
Three international multicenter phase II trials were initiated in 1999.
The study population included patients with CML in myeloid BC, relapsed
Ph+ALL, CML in AP, and patients who were resistant to IFN alpha. The
results achieved in patients suffering from BC with myeloid phenotype
largely confirmed the results obtained in the phase I study.[9] In
contrast to patients with myeloid type of disease, none of patients
treated for lymphoid blast crisis and for relapsed Ph+ALL had durable
response to imatinib.[10]
The results of patients treated
for AP fall between those observed in myeloid BC and CP with the 1-year
survival achieved in 74% patients. A retrospective comparison between
two dose cohorts (400 mg and 600 mg daily) showed a significantly
longer time to progression and overall survival for the 600 mg
cohort.[11] Based on
these studies the recommended daily dose
for patients in advanced phases of CML was set at 600 mg daily,[9,11]
and the recommendation of increasing the imatinib dose to 600 and 800
mg daily was rapidly extended also to patients in CP with
unsatisfactory response to 400 mg daily, or response
loss.
The patients suffering from CML in CP hematologically or
cytogenetically resistant or refractory, or intolerant of IFN alpha
were the largest group studied within phase II trials. Ninety five
percent of all patients achieved CHR; CCyR and MCyR were seen in 41%
and 60% of patients respectively, and the progression-free survival
rate at 18 months was 89%.[6]
Phase
III trials:
An International Randomized Study of Interferon and STI571 (IRIS)
comparing imatinib at a single daily dose 400 mg to IFN alpha plus
cytarabine in newly diagnosed patients with CML in CP was initiated in
June 2000. Results from this study show the outstanding effectiveness
of imatinib and its superiority with respect to the rates of CHR, MCyR
and CCyR. At 18 months, the rate of CCyR in patients treated with
imatinib was 76% versus 15% for patients treated with IFN alpha plus
cytarabine (P<.001). Importantly, the rate of progression to AP
or
BC at 18 months was significantly reduced in patients randomized to
imatinib arm.[12] Based on these
results, the FDA has approved imatinib
as first-line treatment for newly diagnosed CML in December 2002. At 8
years of follow-up, 45% of patients had discontinued treatment due to
adverse events (AEs)/safety (6%), unsatisfactory therapeutic outcome
(16%), stem cell transplantation (SCT) (3%), death (3%) or other
reasons (17% for withdrawal or lack of renewal of consent and
miscellaneous). Patients randomized to imatinib arm at 8 – year data
cut off continue to have a durable hematologic and cytogenetic
responses, low progression rates to AP or BC, and remarkable survival
outcomes.[12-15] An overall
survival (OS) rate is 85% for
patients receiving imatinib (93% when only CML- related
deaths
and those prior to stem cell transplantation are considered), with the
annual rates of progression to AP or BC in year 4 to 8 after imatinib
therapy onset are: 0.9%, 0.5%, 0%, 0%, and 0.4%, respectively.
Progression to AP or BC was noted only in 3% of patients who achieved
CCyR, and in none of patients who achieved major molecular response
(MMR, <0.1% BCR-ABL/control gene ratio on international scale)
at 12
months of therapy.[16] The
patients treated with imatinib who had at 18
months a ≥3 log reduction in the level of BCR-ABL transcripts compared
with a standardized baseline had a minimal risk of disease progression
over the subsequent 12 months.[17]
The achievement of an MMR continued to be associated with an improved
outcome at 5-year, with estimated rates without progression to AP/BC of
100%, 98%, and 87% for patients achieving CCyR and MMR, CCyR without
MMR, and no CCyR, respectively.[13]
The best observed MMR rate with the
8-year follow-up of IRIS trial is 86%. The results of imatinib first
line based on analysis of data derived from clinical trials and
registries have been reported in the last three years by several groups
(PETHEMA, SPIRIT, GIMEMA, CAMELIA, German Study Group IV, and
others.).[21-30] The rates of CCyR
achieved after one year of therapy
with imatinib at standard dose ranged from 49% to 77%, and the
proportion of patients who achieved MMR after one year ranged between
18% and 58%.
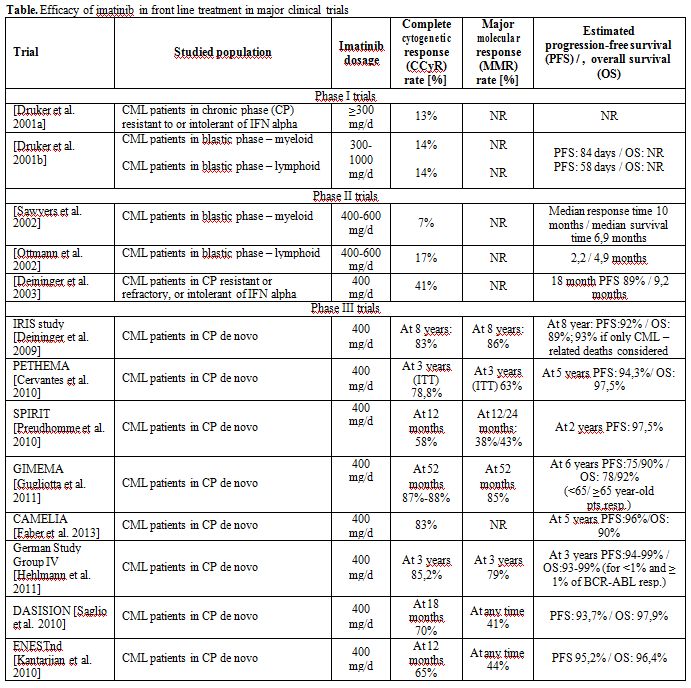
| Table 1. Efficacy of imatinib in front line treatment in major clinical trials |
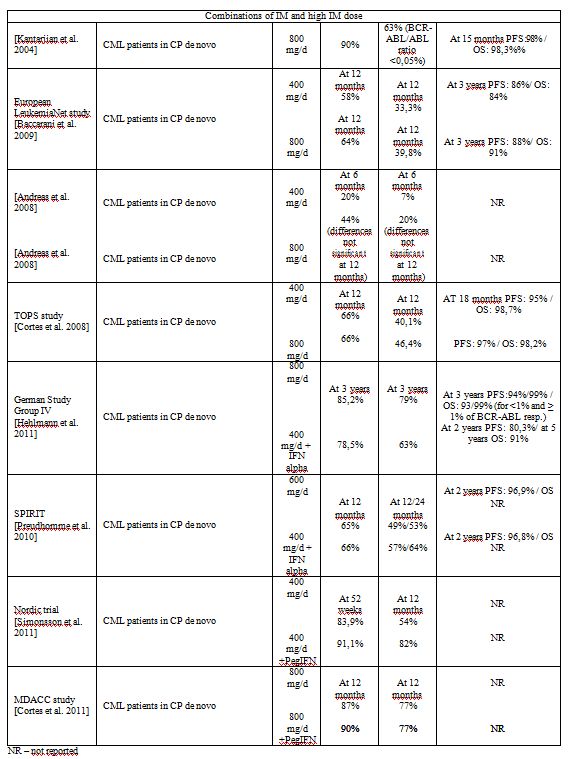
The Efficacy of Imatinib at Higher Dose; Combinations with other Agents
Preclinical data and some observations from single – arm studies suggested that higher dosages of imatinib could be more effective than standard 400mg once daily dose, and may provide a better disease control. The amplification of the BCR-ABL gene or overexpression of bcr-abl protein kinase are two known mechanisms of relative resistance to imatinib[34-36] which could be overcome by dosages of 600 mg or 800 mg daily. However the initial reports that high dose imatinib treatment results in better, and achieved more rapidly responses than during standard dose imatinib remain controversial. Kantarjian et al. reports that compared with standard-dose imatinib, the dose of 800 mg daily was associated with achievement of significantly better rates of CCyR, major (defined as BCR-ABL/ABL ratio ≤0.05%), and complete (BCR-ABL/ABL negative) molecular responses. Transformation-free survival in this cohort of patients was significantly better with high-dose imatinib. Similar frequency of common adverse events with that seen with standard-dose imatinib was reported. The most common causes for dose reduction were myelosuppression.[37] The German Study Group IV randomized trial compared imatinib 800 mg daily with standard dose imatinib +/- IFN in newly diagnosed CML patients in CP with regard to molecular response at 12 months and survival. Of 218 patients receiving imatinib 800 mg and evaluable for dosage at 12 months 45.9% received more than 700 mg/day. The cumulative incidences of CCyR and MMR at 12 months were significantly higher in imatinib 800 mg arm and lower and comparable in imatinib 400 mg and imatinib 400 +IFN alpha arms. MMR at 12 months have been reached faster with imatinib 800 mg, but this faster response did not translate into a better OS or progression-free survival (PFS).[25] A Randomized European LekemiaNet Study addressed the issue of comparison of imatinib 400 mg and 800 mg daily in the front-line treatment of high-risk, Philadelphia-positive CML patients. 216 high risk patients according to the Sokal index were randomized into a group treated for at least 1 year front – line with imatinib at a dose of 800 mg daily or 400 mg daily. At 12 months the rate of CCyR (the primary endpoint) was better in the high-dose arm than in the standard-dose arm but the difference was not statistically significant. Importantly, the number of failures and the number of patients who discontinued treatment for any reasons were not different in those two arms. The proportion of MMR at any time point was slightly but nonsignificantly higher in the high-dose arm than in the standard-dose arm. This large, prospective, intention-to-treat, randomized study on therapy for high risk patients with CML failed to demonstrate a benefit of imatinib administered at a higher dose for the primary end point, as well as for any other measure of efficacy, toxicity, and compliance.[38] In the other study of imatinib 400 mg versus 800 mg daily in 227 patients in late chronic phase who were resistant or intolerant to IFN alpha imatinib 800 mg daily was associated with a higher CCyR rate at 6 months but not at 12 months.[39] The MMR rate at 12 months was the primary end point of another study of 476 patients, any risk, who were randomized to receive front-line imatinib at a dose of 800 mg or 400 mg daily.[40] The difference in the MMR rate at 12 months between 400 mg and 800 mg arm was not significant. These studies do not support the wide use of imatinib at higher dosis front-line in all patients suffering from CML.
Combination of imatinib with low dose arabinosyl cytosine have been tested in two randomized trials, but none have demonstrated a superiority versus therapy with imatinib alone.[41,22] The German CML Study IV was designed to compare in a randomized fashion standard imatinib vs. imatinib + IFN alpha vs. imatinib + low dose araC vs. imatinib after IFN (for low- and intermediate-risk patients) or vs. imatinib 800 mg (for high-risk patients). At 3 years, the cumulative incidence of CHR, MCyR, CCyR and of MMR were comparable for primary imatinib therapies.[41] A French SPIRIT randomized study for untreated chronic-phase CML patients compared efficacy of imatinib alone at a dose of 400 mg daily, imatinib (400 mg daily) plus cytarabine (20 mg per square meter of body-surface area per day on days 15 through 28 of each 28-day cycle) or pegylated interferon (peginterferon) alfa-2a (90 μg weekly), or imatinib alone at a dose of 600 mg daily.[22] At 12 months, the rates of CCyR were similar among the four groups. Combination of imatinib and low dose arabinosyl cytosine was not superior to imatinib alone in any measure of efficacy. Patients treated with combination of imatinib and peginterferon alfa-2a achieved significantly better rate (30%, 38%) of a superior molecular response (corresponding to MR 4) than patients receiving 400 mg of imatinib alone (14%, 21%) at 1, and at 2 year respectively (P = 0.001). During the first year of the trial, however, 39% of the patients discontinued cytarabine, and 45% discontinued peginterferon alfa-2a, both predominantly due to a toxicity. A lower dose of peginterferon alfa-2a (e.g., 45 μg per week) enhanced the tolerability while retaining the antileukemic efficacy. The rate of grade 3 to 4 hematologic toxicity has been reduced from 54% to 27%, and the proportion of patients who discontinued peginterferon alfa-2a before 6 months decreased from 40% to 10%. By 12 months, the cumulative MR4 for the subgroup treated with imatinib at a dose of 400 mg and the PegIFN90 vs imatinib of 400-mg and PegIFN45 were 25% and 28% respectively.[42] The main phase of CML German Study IV compared monotherapy with imatinib 400 mg/d versus imatinib 400 mg/d combined with nonpegylated IFN-alpha given at an initial dose of 1.5 mill.U three times per week and increased up to 3 mill.U three times per week, according to tolerability versus imatinib 800 mg/d. At 12 months the rates of MMR which was the first primary end point were similar in the monotherapy imatinib 400 mg/d arm (44% [95% CI, 37% to 50%]) and in the imatinib 400 mg/d combined with IFN-alpha 46% [95% CI, 40% to 52%] arm and inferior to imatinib 800 mg/d arm.[25] In the Nordic trial newly diagnosed chronic-phase CML patients with a low or intermediate Sokal risk score were randomized either to group treated with a combination of pegylated IFN-alpha 2b (Peg–IFN-alpha 2b) at a dose of 50 µg weekly and imatinib 400 mg daily or with imatinib 400 mg daily as a monotherapy. The MMR rate at 12 months was significantly higher in the combination arm (82%) compared with the imatinib monotherapy arm (54%; intention-to-treat, P=.002). In the combination arm, however, 61% of patients discontinued Peg–IFN-alpha 2b, most because of toxicity.[43] In the MD Anderson Cancer Center (MDACC) trial patients were randomized to receive imatinib 400 mg twice daily, and combination of imatinib 800 mg/d with pegylated rIFN-alpha 2b 0.5 μg/kg weekly. The MMR and the CCyR rates were comparable in both arms.[44] None of these combination studies has demonstrated a superior PFS or OS for patients who received combined treatment.
Studies on Cessation of Imatinib
Allogeneic – haematopoietic stem cell transplantation (Allo-HSCT) has
been and is still considered as the sole treatment able to cure CML. As
a result of allo-HSCT a long period of time free from cytogenetic or
hematologic relapse of the disease without the need for maintenance
therapy could be achieved.[45,46]
However a thorough monitoring of
minimal residual disease with qRT-PCR could demonstrate a presence of
the BCR-ABL gene transcript even a long time after transplantation,
which does not necessarily imply relapse, because no other signs of
disease recurrence were observed.[47,48]
Apparently most of the
patients were cured even though not all BCR-ABL positive leukemic cells
were completely eradicated. A similar pattern is now observed in the
course of the long-term follow-up of TKI-treated patients who
eventually stop the treatment after achieving a deep and sustained
molecular remission, and is a convincing illustration of the concept of
„operational cure”.[49] The first
pilot study was initiated in 12
chronic phase CML patients treated with imatinib at a standard dose who
have achieved and maintained a complete molecular response (CMR) for at
least 2 years, which was assessed by qRT-PCR with a sensitivity ranging
between a 4.5- and a 5-log reduction. After a median follow-up time of
18 months, 50% of patients remained off-therapy without reappearance of
BCR-ABL transcripts.[50] Those
patients still have an undetectable
level of BCR-ABL transcripts after a median follow-up time of 6 years
(range, 4-8). The same entry criteria were used for the multicenter
study entitled the “Stop Imatinib” (STIM) which enrolled prospectively
one hundred patients. The treatment with imatinib was restarted in the
case of molecular relapse, which was arbitrarily defined as 2 positive
qRT-PCR results over a period of 1 month showing at least a 1 log
increase in BCR-ABL transcripts. At 36 months the overall probability
of molecular relapse–free, and treatment-free remission was 39% (95%
CI, 29-48). Most patients relapsed within 6 months from imatinib
cessation; 3 cases of late relapse occurring at months 19, 20, and 22,
respectively were noted. Most patients form the pilot as well as from
the STIM study remained responsive to retreatment with imatinib. The
second French “Stop Imatinib” (STIM2) study used the same criteria as
those for the STIM1. The molecular relapse was defined also in a
similar way, and a loss of MMR detected at one point was a trigger of
TKI retreatment. The median follow-up of 124 enrolled patients is 12
months (range 1-25). After discontinuation of imatinib, a molecular
relapse occurred in 48 pts (most within 6 months form imatinib
cessation; 3 relapses between 6 and 12 month), and 76 patients (61%)
were still free-of treatment at the last update. Forty one patients
experienced a BCR-ABL transcript fluctuation in the qRT-PCR without
clear molecular relapse.[52] The
TWISTER study is a prospective
clinical trial which have used very similar as those in a STIM study
entry and molecular relapse criteria for 40 chronic phase CML patients
who discontinued imatinib. At 24 months, the proportion of patients
remaining in stable treatment-free remission was 47.1%. Most patients
relapsed within 4 months of stopping imatinib, importantly, no relapses
beyond 27 months were observed.[53]
Other report demonstrates the
probability of maintaining the CMR at 1 year of 28,6% after
discontinuation of imatinib in 14 chronic phase CML patients. None of
the patients however was strictly in CMR throughout the entire 2-year
period preceding cessation of imatinib and half of the patients were
high risk according to the Sokal index.[54]
A nationwide survey
conducted in Japan identified 50 patients who stopped imatinib for at
least 6 months. Molecular relapse was detected in 19 out of 43 analyzed
patients, and the CMR rate after imatinib discontinuation was estimated
to be 47%.[55] All mentioned above
studies demonstrate the proof of
concept for stopping imatinib in CML patients who were able to achieve
a deep, sustained molecular response. It seems certain that an MMR is
not enough to plan a discontinuation strategy. The STIM1 and STIM2
study used a 4.5 – 5-log reduction, and the TWISTER study used a
4.5-log reduction for their definition of CMR. Larger studies suggest
that beside of the level of BCR-ABL transcripts after imatinib
treatment, the duration of deep molecular response is of major
importance in achievement of a long-term treatment-free survival. In
the STIM1, STIM2 and TWISTER trials, a sustained CMR for at least 2
years was used as the criterion.[51-53]
In the multivariate analysis
and logistical regression in the STIM1 study, Sokal risk and imatinib
therapy duration were confirmed as 2 independent prognostic factors for
prediction of molecular relapse after imatinib discontinuation.[51] It
is obviously necessary to monitor regularly the minimal residual
disease using qRT-PCR to allow an early detection of a fast molecular
recurrence and restart the treatment as soon as possible. Most of the
molecular recurrences occurred within the first few months of imatinib
cessation. The presence of residual BCR-ABL positive cells in CML
patients in CMR before and after imatinib discontinuation were
demonstrated by Ross et al. who used genomic DNA-based PCR, which
allows to detect rearranged BCR-ABL gene at a level of around 1- to
2-log below the detection limit of conventional (mRNA) qRT-PCR.
However, there was no link between detection of BCR-ABL by genomic
DNA-based PCR and relapse.[53]
Monitoring of residual disease by more
sensitive conventional qRT-PCR within STIM1 study also does not allow
the prediction of relapse after imatinib cessation.[51]
Importantly
some fluctuations in BCR-ABL levels detected by conventional qRT-PCR
method (in 33% patients in STIM2 study) could be observed after
discontinuation without confirmation of a molecular relapse. 41
patients (33%) in STIM2 study experienced a BCR- ABL qRT-PCR
fluctuation without molecular relapse, confirming that BCR-ABL
reappearance does not mean automatically clinical relapse and
reinforcing the concept of “operational cure”.
[9]
References
[TOP]