Received: June 3. 2014
Accepted: July 2, 2014
Meditterr J Hematol Infect Dis 2014, 6(1): e2014053, DOI 10.4084/MJHID.2014.053
This article is available on PDF format at:

Annarosa Cuccaro, Francesca Bartolomei, Elisa Cupelli, Eugenio Galli, Manuela Giachelia and Stefan Hohaus
Institute of Hematology, Catholic
University S. Cuore, Rome, Italy.
|
This
is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract Hodgkin
lymphoma (HL) is among the neoplastic diseases that has the best
long-term outcome after cytotoxic treatment. Cure rates approach
80-90%; however, 15-20% of patients will be resistant to therapy
(primary refractory) or relapse after treatment. Prognostic factors
should help to stratify treatment according to the risk profile and
identify patients at risk for failure. Significance of prognostic
factors partly depends on the efficacy of the treatments administered,
since new effective therapies can variably counterbalance the adverse
effects of some unfavorable clinical determinants. As a consequence,
some prognostic factors thought to be important in the past may become
meaningless when modern successful therapies are used. Therefore, the
value of prognostic factors has to be updated periodically, and then
adapted to new emerging biomarkers. Besides the prognostic role of PET
imaging, tissue and circulating biomarkers, as the number of
tumor-infiltrating macrophages, cytokine and chemokine levels and
profiling of circulating nucleic acids (DNA and microRNAs) have shown
promise.
|
Introduction
Treatment of Hodgkin lymphoma (HL) is
an indubitable one of the greatest success stories of medical oncology
in the 20th
century. Cure rates approach 80-90% of patients, and HL is among the
neoplastic diseases that have the best long-term outcome after
cytotoxic treatment. However, 15-20% of patients will be resistant to
therapy (primary refractory) or relapse after treatment, usually in the
first two years. This review will analyze the prognostic factors that
can identify patients at risk. Since outcome of patients is determined
not only by disease characteristics but also by the risk of short- and
long-term sequelae of the treatment, which can even outnumber the
events of disease recurrence, the identification of risk factors for
secondary events will be increasingly important to tailor the therapy
and thus avoiding potential harmful treatments in individuals at risk.
In a simplified way, prognostic factors can be divided into areas that
are related to the disease, factors related to the patient as a host
for the disease and to the therapy (Figure
1).
Interactions between these areas exist. The genetic background of the
patient is a host factor that modulates the metabolism of cytotoxic
drugs, and as a consequence alters the response and side effects of the
treatment.
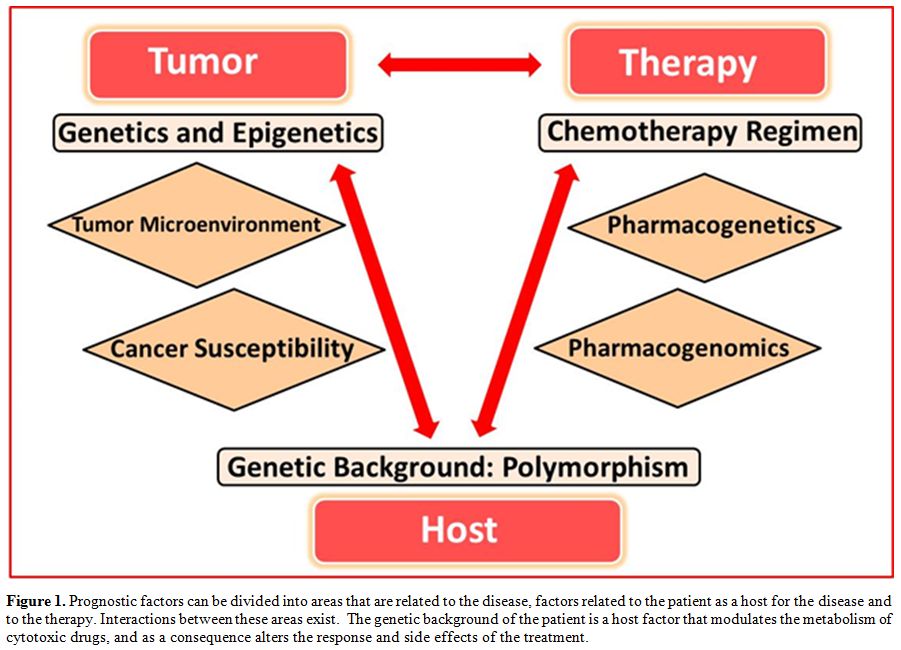 | Figure 1. Prognostic factors can be divided into areas that are related to the disease, factors related to the patient as a host for the disease and to the therapy. Interactions between these areas exist. The genetic background of the patient is a host factor that modulates the metabolism of cytotoxic drugs, and as a consequence alters the response and side effects of the treatment. |
In
this review, we will only briefly discuss the prognostic relevance of
pathological and immunological features of HL, and not consider PET
imaging, that has evolved into the most exciting tool to evaluate the
prognosis in HL in recent years. This topic will be covered with
another review in this issue of the journal. Many prognostic factors,
used in standard clinical practice, have been known for a long time.
These factors often reflect disease burden and disease activity that is
related to the inflammatory microenvironment. Biomarkers described in
recent years are indicators of the disease activity as well, but they
describe this activity in a more sophisticated, accurate and
pathogenetically more relevant way. Often these new prognostic factors
still need validation, but they may eventually substitute for classical
clinical factors.[1]
Tumor Burden: Stage and Bulk
Extension of disease and tumor burden is indubitable the most important disease characteristic, that is used to stratify treatment strategies (Figure 2). Staging according to the Ann Arbor system is part of clinical routine for more than 40 years.[2] In limited stage disease, the presence of bulky disease detected on chest radiography or CT at staging is considered a negative predictor of outcome. The presence of a bulky tumor is one of the risk factors in the European Organization for Research and Treatment of Cancer/Groupe d’étude des Lymphomes de l’adulte (EORTC/GELA) and the German Hodgkin Study Group (GSHG) stratification scores for HL.[3] By contrast, in advanced stage disease, the presence of a bulky tumor is not a risk factor in the international prognostic score (IPS) for HL.[4] Since measurement of bulk is limited to the single largest mass, it could underestimate the total tumor burden in patients with diffuse disease. Newer methods to measure tumor burden with CT volume or metabolic tumor volume may give more precise estimation of the tumor volume.[5-7] Normalization of the tumor mass to the body surface (the relative tumor burden) yields a parameter with a reliable prediction for tumor control modulated by the use of chemotherapy regimens with different intensity.[7] The complexity of the evaluation of all lesions in any scan slice with subtraction of normal structures that are present in the tumor tissue, and approximation for bone marrow involvement has limited a wider application of this type of evaluation. Therefore, an indirect estimate was derived from a few staging parameters and demonstrated sufficient statistical reliability when compared with the direct measure of rTB.[8] The equation {Estimated rTB = −4.3 + 8.3 × IPI2+ 22.7 × [number of involved sites (+3 if bulky mass is present)]} was recently proposed for investigational and clinical uses when the direct measurement cannot be performed.
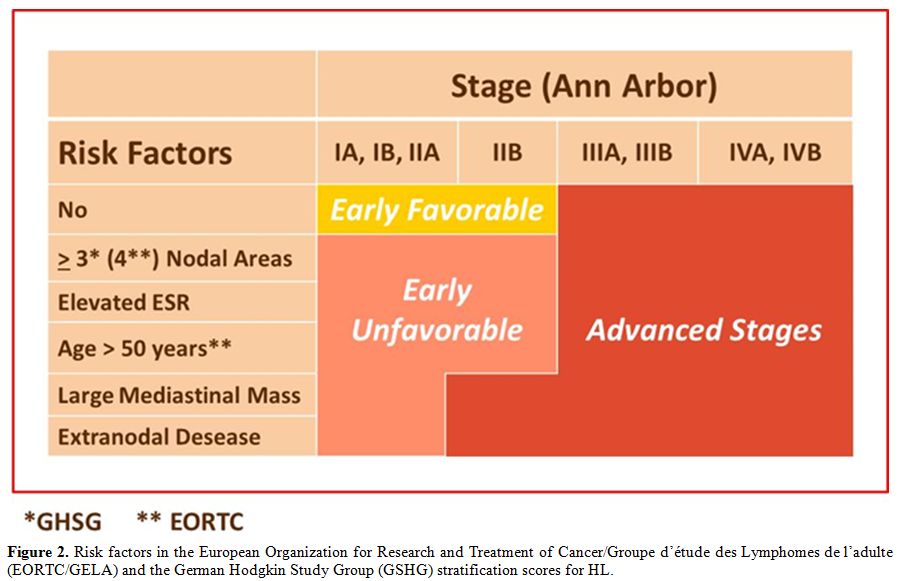 | Figure 2. Risk factors in the European Organization for Research and Treatment of Cancer/Groupe d’étude des Lymphomes de l’adulte (EORTC/GELA) and the German Hodgkin Study Group (GSHG) stratification scores for HL. |
Spread
of HL beyond its lymph node microenvironment to extralymphatic organs
is associated with inferior outcome. In limited stage disease
involvement of an extranodal site is defined as a risk factor by the
GSHG scoring system. In patients with advanced-stage disease, diffuse
organ involvement defining stage IV disease is an independent risk
factor in the IPS.[9]
Age
Age is the most important factor when overall survival is analyzed, and
remains an independent factor also for progression-free survival. It
impacts on prognosis in at least two ways: On one hand, it is
intrinsically associated with HL biology and, on the other hand, older
age often is associated with co-morbidity and reduced tolerability of
chemotherapeutic regimens used in younger patients. HL epidemiology is
characterized by a bimodal age distribution. Following the peak in
young adults in their twenties, there is a second increase in the
incidence, in particular in males, after the age of 50-55 years. When
compared to other hematological neoplastic diseases, that usually set
the cut-point to define elderly patients at 60 years, the prognostic
cut-point in HL is shifted versus a younger age.
In the International Prognostic Score for patients with advanced stage
disease the cut-point is age of 45 years, the EORTC lists age more than
50 years as a risk factor for patients with limited stage disease.
Older age associates with a higher frequency of the mixed cellularity
histotype and presence of EBV in the neoplastic cells, when compared to
younger patients.[10]
EBV-association appears to be a prognostic factor that is limited to
the elderly patients.[11-13]
It is hypothesized that loss of immunological control of EBV-infected
cells might contribute to the development of EBV-associated HL in the
elderly. Aging of the immune system (immunosenescence) is characterized
by reduced function of the adaptive immune response that includes T and
B cell function. Studies are required to address the question whether
immunosenescence is a mechanism in the pathogenesis of elderly HL, and
whether this will contribute to the negative effect of age on
prognosis.
Therapy of HL in the elderly is often complicated by toxic side effects
of chemotherapy. Standard treatment with ABVD is often not recommended
for patients older than 70 years. Bleomycin leads to frequent incidence
of pulmonary toxicity in the elderly. In a recent report, the incidence
of bleomycin lung toxicity was 32% with a 25% mortality.[14]
Intensified regimens as the BEACOPP-dose escalated regimen are not
recommended for patients with advanced-stage HL over 60 years.[15]
However, even in patients over 50 years with reduced performance
status, mortality of BEACOPP-dose escalated increases to 13.3%.[16]
Therapy of elderly patients with HL remains a challenge, and effective
regimen with acceptable toxicity profiles is still lacking. The
availability of antibody-drug conjugates, as Brentuximab may be major
step forward.
Gender
Males with HL have a poorer outcome than females. This effect of gender
is not limited to HL. As well, female patients with follicular lymphoma
and diffuse large B cell lymphoma fare better than their male
counterparts. On the mechanism of the gender effect on prognosis in HL,
one can only speculate, but it could influence prognosis in at least
two ways. A preponderance of male gender is observed in elderly
patients, and as a consequence males have more often unfavorable
disease characteristics. Another mechanism for the gender effect in
lymphoma may be due to differences in pharmacokinetics. Female patient
with HL experiences more hematological toxicity, especially more severe
leucopenia, probably due to gender difference in metabolism of
cytotoxic drugs of the ABVD regimen.[17]
Moreover, hematological toxicity has been associated with a more
favorable outcome.
B-Symptoms
Constitutional symptoms defined by unexplained fever >38°C,
drenching night sweats and weight loss >10% of the weight are a
presenting sign in about 10-25% of patients with limited stage disease,
and up to 70% of patients with advanced stage disease.[9]
Among the symptoms, isolated night sweats do not appear to be
associated with inferior outcome. The presence of B-symptoms is a risk
factor, in particular in stage II bulky disease, that is not considered
to be a limited stage disease by the German Hodgkin study group when
B-symptoms are present.
B-symptoms are due to the production of pro-inflammatory cytokines by
the Hodgkin tumor tissue, in particular IL-1, TNF-alpha, and IL-6.[1]
B-symptoms are associated with a variety of other laboratory
abnormalities and patients’ characteristics, and in multivariate
analyses it has therefore often been removed in final models, as in the
IPS.
Anemia
Anemia is a frequent finding at HL diagnosis and is present in about
40% of patients. It is usually a mild to moderate normocytic anemia,
with the characteristics of anemia of inflammation. Cut-off point for
prognosis in the IPS is a hemoglobin level of 10.5 g/dl, and this is
independent of gender.
We demonstrated that elevated IL-6 levels correlate with hemoglobin
levels and that IL-6 levels correlate with levels of hepcidin, an acute
phase reactant and a major regulator of iron metabolism.[18]
Therefore, anemia is linked to the inflammatory activity of the HL
microenvironment, and this might explain its big prognostic impact.
Anemia of inflammation is characterized by alterations in iron
metabolism. Elevated production of hepcidin blocks the release of iron
from the intestine and iron stores in the reticuloendothelial system
that results in increasing levels of ferritin. Elevated ferritin levels
have been described in HL and have been associated to prognosis four
decades ago.[19] The accumulation
of iron also in the
HL microenvironment can have biologic effects on cell function and
induce cell damage by induction of reactive oxygen species (ROS) that
interfere with the function of macromolecules as DNA, and proteins.
The White Blood Cells: Leukocytosis, Lymphopenia, Monocytosis
Alterations of the counts and composition of the white blood cells in
peripheral blood are often at diagnosis in HL and well known prognostic
factors. Typical alterations in WBC counts include leukocytosis with
neutrophilia, lymphocytopenia, either relative or absolute, and
monocytosis.
In the IPS the prognostic cut point for white blood cell count is set
at 15000/microL, for lymphocytopenia it is 600/microL or less than 8%.[9]
More recently, the monocyte count, in particular in relation to the
lymphocyte count has been reported to be a prognostic factor in HL and
other lymphomas.[20] In a case
cohort of 474 patients
with HL observed from 1974 to 2010, monocyte count of
>900/microL
was associated with inferior progression-free and overall survival. The
impact of the monocyte counts on prognosis became particularly evident
when the ratio between lymphocytes and monocytes (ALM ratio) was
<
1.1. As the number of macrophages in the HL tissue is strongly
associated with prognosis, the question arises whether the number of
monocytes in PB and the number of tumor-associated macrophages (TAM)
are correlated.
Albumin
Low levels of serum albumin are associated with a worse prognosis in
many hematological neoplasias, including HL. The IPS score defines
albumin levels of 4.0 g/dl as cut-point. Albumin is produced by the
liver, and about 12-20% of the protein synthesis capacity of the liver
is dedicated to albumin production. Albumin synthesis is reduced when
synthesis of acute-phase proteins is stimulated by IL-6 or when
availability of amino acids is decreased due to reduced nutritional
status. Albumin levels inversely correlate to IL-6, TNF alpha and
IL1-RA.[1]
The Erythrocyte Sedimentation Rate
The erythrocyte sedimentation rate, albeit its nonspecific character is
one of the oldest prognostic factors for HL. It is still in use to
define early stage HL as favorable or unfavorable. The EORTC and GSHG
set the cut-point to 30 mm/h for patients with B –Symptoms and 50 mm/h
for patients without B-symptoms. The ESR is increased in many diseases,
in particular in those with an inflammatory reaction. The ESR can be
altered by many variables, as the erythrocyte count and the protein
composition in the plasma, in particular increased levels of
fibrinogen, acute phase proteins and gamma globulins can increase the
ESR. As these parameters are as well prognostic markers in HL, the ESR
does often not maintain its value in multivariate analysis.
Beta2-microglobulin
B2M is a component of the HLA-I antigen and present on the surface of
nearly all nucleated cells in the body. In healthy people, it is
produced at a constant rate and eliminated in the kidney where free
glomerular filtration is followed by tubular re-adsorption. Lymphocytes
are the main production site of b2M, and inflammatory cytokines
stimulate the production of b2M, and increased levels of b2M can be due
to increased release from immune system activation or proliferation or
decreased renal clearance. It is a prognostic marker in many lymphomas,
including HL. Elevated levels of B2M can be found in 5-30% of patients
at diagnosis, depend on the stage, and have been found to be associated
with the relapse.[21-23]
Biohumoral Factors: IL-10, IL-6, sCD30, TNF, TARC
A large array of cytokines can be detected at increased levels in
peripheral blood in HL. These are produced both by the HRS cells and
the surrounding microenvironment. The prognostic significance of
cytokine levels has been studied for more than 20 years in HL, and the
most frequently studied cytokines are IL-10, IL-6, TNF alpha and its
soluble receptors, and more recently the chemokine TARC. IL-10 is of
particular interest in the immunopathogenesis of HL, as it is supposed
to play an important role in the shift of T cell function from Th1 to
Th2 and Treg functional state. IL-10 levels are elevated in about
40-50% of patients, and associate with inferior outcome.1,[24-30] IL-10 levels appear to be higher
in EBV-associated HL.[29]
IL-6 is a pro-inflammatory cytokine that is associated with some
clinical and laboratory manifestations of HL, as, B-symptoms, anemia,
and low albumin levels.[31] IL-6
can induce the
production of hepcidin, a major regulator of iron metabolism and
mediator for anemia of inflammation or chronic disease, characterized
by iron-restriction. We showed that IL-6 – hepcidin axis is active in
anemia associated with HL, but that other IL-6-induced,
hepcidin-independent mechanisms probably play a role.[30]
The circulating CD30 antigen sCD30, is thought to be shed form the
CD30+ HRS cells, and represents, therefore, at least theoretically, an
ideal tumor marker for the neoplastic cells. sCD30 levels are increased
in about 25-30 % of patients with HL, and, levels above 100 -200 U/ml
associate with worse outcome.[32]
Ma et al.[33] used a proteomic
approach to screen for
proteins in plasma at HL diagnosis to identify new protein biomarkers.
The most promising biomarkers appeared to be TARC (thymus and
activation-regulated chemokine), a chemokine that is important for
attracting immune cells with specific functions to the microenvironment.
The chemokine TARC has recently attracted more interest as it plays a
central role in the composition of the microenvironment attracting Th2
and Treg cells. TARC levels are elevated in the vast majority of
patients with HL at diagnosis, and rapidly turn to normal during
treatment.[34-35] Preliminary data
indicate an
association between changes in TARC concentration in plasma and therapy
outcome. Whether this early change can be a marker to evaluate response
has to be addressed in larger studies.
Casanovas and colleagues developed a prognostic score based on
different cytokine levels.[1]
The score included IL-6, sCD30 and TNFR1 and was more predictive than
standard clinical score. While this work is of high interest, these
data need confirmation on independent data sets and in relation to the
results of early or interim PET.
Prognostic Relevance of Characteristics of HRS Cells
The number and atypia of HRS cells together with the degree of
cellularity in the nodules and the amount of sclerosis are the
characteristics for the separation of nodular sclerosis (NS) into grade
1 and grade 2 according to the British National Lymphoma Investigation
(BNLI)[].[36] NS grade 2 typically
is more
aggressive, and has an inferior outcome. However, difficulties to
reproduce this classification has resulted in conflicting data and
limited the widespread use of this classification.[37-38]
Several studies indicated that BCL-2 expression in HRS cells is
associated with an inferior prognosis.[39-41]
However, the relationship between BCL-2 expression and patient outcome
in HL remains controversial because other studies have not demonstrated
the same correlation between bcl-2 expression and failure-free
survival.[42] Similarly, the
association of p53 with patient outcomes in HL remains controversial[40-42] although more studies suggest a
prognostic role for BCL-2 than for p53.
Prognostic Relevance of the Tumor Microenvironment
HL is characterized by an expansion of T cells with a T helper2 and T
regulatory phenotype in the microenvironment. However, both
immunohistochemistry and gene expression studies indicate that high
numbers of T cells with a cytotoxic phenotype and low numbers of FOXP-3
+ T reg cells in the microenvironment are associated with inferior
outcome.[43-45] A number of other
components in the
microenvironment as, B cells and eosinophils have been reported to be
associated with prognosis.[46-47]
However, this information is not part of the routine evaluation for the
prognostic purpose.
A more recent tissue biomarker is the number of tumor-infiltrating
macrophages, identified by immunohistochemical staining for the CD68
antigen,[48] which is a relatively
simple tissue biomarker of gaining widespread interest.[49]
However, not all studies could confirm the prognostic impact of the
count of tumor-associated macrophages in HL. Further studies are needed
to determine the optimal antigen (e.g. CD68 versus CD163), anti-CD68
antibody clone (e.g. KP1 versus PGM1) and scoring thresholds (e.g.
manual versus computer-assisted) for detecting HL associated
macrophages.49 The Vancouver group developed a 23-gene outcome
predictor that was superior to the IPS and to CD68
immunohistochemistry.
Circulating DNA of Cellular and Viral (EBV) Origin
Cell-free DNA of cellular and viral origin can be detected in the
plasma of patients with HL at diagnosis.[50-51]
Cell-free DNA is released from the tumor tissue, and levels correlate
to disease activity.[52]
Cell-free DNA is probably released both by the tumor cells and the
surrounding microenvironment. The identification of recurrent mutations
in patients with HL opens the possibility to develop sensitive
techniques to detect these mutations in the cell-free DNA fraction as
specific tumor markers in the peripheral blood.[52-53]
Patients with cell-free DNA levels above the normal range have an
inferior event-free survival.[50]
In the same line, EBV-DNA can be detected in the plasma of patients
with HL, and represents a marker for the activity of EBV-associated HL.[54]
It is important to underline that detection of EBV in plasma, but not
in the mononuclear cell fraction is associated with the EBV-status in
HL.[51,54]
We and others have shown that the presence and level of EBV-DNA is a
prognostic marker. [51,54-55]
Genetic Background
Genome-wide association studies (GWAS) on large cohorts of patients
with HL have defined the role of polymorphic germ line variants as a
risk factor for the development of HL.[56-58]
These
studies commonly identified a locus on chromosome 6 in the HLA region
as a highly significant risk allele for HL. Other single nucleotide
polymorphisms, in other HLA regions and cytokine genes, as IL-13 have
also been associated with HL risk. About the role of the genetic
background as a factor that can modulate the response to treatment and
outcome of patients with HL, no results of GWAS are available. Using a
target gene approach, we and others reported on the prognostic impact
of SNPs in HL. Most of genes studied were involved in the metabolism of
cytotoxic drugs, as detoxification enzymes, and immunoregulatory genes,
given the pivotal role of immunological alterations and interactions in
the pathology of the disease.[59-66]
In particular,
we found deletions of GSTT1 and GSTM1 and a variant in the GSTP1 gene
(Val105Ile), which reduces the enzymatic activity, be associated to a
better outcome.[59-60] These data
could only be
partially confirmed on an independent cohort of patients with advanced
HL included in multicenter trial.[67]
Other studies
reported on the prognostic impact of genes coding for enzymes involved
in drug metabolism are and UGT1A1 and GSTA1.[61,64]
We reported that carriers of variants in the promoter region of the
IL-6 and IL-10 genes that are supposed to influence gene expression
were associated with prognosis in HL.[68]
Validation
on independent and large patient cohorts is needed before the germ line
variants in the genetic background can be clinically used to modulate
the treatment.
Prognostic Scores
Clinical and laboratory parameters have been combined into different
prognostic scoring systems. Patients with limited stage disease are
traditionally divided into a favorable/unfavorable group according to
the presence of risk factors defined with some minor differences by the
GSHG and EORTC (Figure 2).[69]
Both GSHG and EORTC use this classification to design treatment
protocols that adapt therapy intensity according to the risk group.
Hasenclever et al. used the data on 5141 patients with advanced stage
disease treated with ABVD or COPP-ABVD to develop a 7-point score
(international prognostic score, IPS). In order to stratify patients
with advanced stage disease, patients are divided into two risk groups
(IPS 0-2 vs. IPS 3-5). However, stratification of therapy according to
Hasenclever score has not entered clinical routine.
Risk scores have also been developed for patients with relapsed
disease. Risk factors as early relapse within 12 months, presence of
B-symptoms and extranodal disease are the most important clinical
factors, as anemia appears to be the most significant laboratory
anomaly to predict poor outcome in relapsed patients.[67,69]
Conclusions
In conclusion, a plethora of prognostic factors is available in HL.
Traditional clinical and laboratory prognostic factors often represent
a surrogate marker for biological characteristics that often are not
included in the standard evaluation. There is no current consensus on
how to integrate these biological markers with accepted clinical
prognostic risk factors into prognostic scores or how to use this
information to adapt treatment. It remains a challenge to identify the
best parameters to predict prognosis in the single patient and identify
the still significant group of patients for whom standard treatment is
not sufficient.
References

[TOP]