Received: June 20, 2014
Accepted: October 7, 2014
Meditter J Hematol Infect Dis 2014, 6(1): e2014069, DOI 10.4084/MJHID.2014.069
This article is available on PDF format at:

Luciana Teofili1, Maria Bianchi1, Bruno A. Zanfini2, Stefano Catarci2, Rossella Sicuranza2, Serena Spartano1, Gina Zini1 and Gaetano Draisci2
1 Hematology Department, Università Cattolica del Sacro Cuore, Rome, Italy
2 Anesthesiology Department, Università Cattolica del Sacro Cuore, Rome, Italy
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background: We retrospectively investigated
the incidence and risk factors for transfusion-related acute lung injury
(TRALI) among patients transfused for post-partum hemorrhage (PPH). |
Introduction
Postpartum hemorrhage (PPH) constitutes the most frequent cause of maternal mortality in low-income countries.[1]
In developed countries, PPH is the prevalent cause of critical illness
among obstetric patients, and recent evidences suggest that its
incidence is progressively rising.[2,3] In particular,
women with persistent PPH, defined as “the active bleeding exceeding
1000 ml within 24 hours following delivery, that continues despite the
use of initial measures including first-line uterotonic agents and
uterine massage”, are considered at high risk of adverse outcome.[4]
Transfusion-related acute lung injury (TRALI) is a serious transfusion
reaction characterized by non-cardiogenic lung oedema, hypoxemia and
respiratory distress occurring after blood transfusion.[5-7]
The reported incidence of TRALI greatly differs in retrospective and
prospective studies: overall, it is estimated to vary between 0.08% and
15% of patients receiving a blood transfusion.[5]
According to the two-hit hypothesis, TRALI results from a capillary
leak caused by two consecutive events: the adhesion of primed
neutrophils to pulmonary endothelial cells (first hit) and, the
subsequent activation of both cells by antibodies or inflammatory
mediators present in transfused blood (second hit).[8]
Antibodies to class II- human leukocyte antigens and to human
neutrophil antigens, contained in donations from persons with a history
of transfusions or previous pregnancies, are often implicated in the
antibody-mediated TRALI.[8] Moreover, various
substances accumulated during the prolonged storage of RBC or PLT are
suspected to elicit antibody-negative TRALI.[8] TRALI
is particularly observed in critically ill patients: massive
transfusion, mechanical ventilation, sepsis, hematological
malignancies, end stage liver disease and cardiac surgery are all
acknowledged important risk factors for TRALI.[9-15]
Since patients with PPH receive transfusion of great amounts of blood
products, it is conceivable that they might be at high risk for
developing TRALI. Therefore, we retrospectively identified a series of
patients heavily transfused for PPH, and we evaluated among them the
incidence and risk factors for TRALI.
Patients and methods
Statistics
Results
Among the 22,344 deliveries occurred at our hospital from January
2005 to December 2011, we identified 71 patients with PPH requiring the
transfusion of at least three RBC units. The mean age + SD was 34 + 5.5
years; 21% of patients had a vaginal delivery and 79% cesarean
delivery. The reported estimated blood loss varied from 300 to 7000 ml.
TRALI diagnosis.
We found evidence of a new-onset hypoxemia within 6 hours after
transfusion in 15 cases: TRALI were identified in 10 of them, possible
TRALI (4 cases) was diagnosed in one patient with pneumonia and in
three patients with pre-eclampsia, whilst in one patient with
pre-existing valvular heart disease, hypoxemia and pulmonary edema were
attributed to transfusion-associated circulatory overload (TACO).[17] Five patients in the TRALI group (36%) and 5 patients in the no-TRALI group (9%) required admission to ICU (p=0.021, Table 2);
overall, no patient required ventilatory support for more than 96 hours
and no patient died. TRALI cases were not notified to the local
hemovigilance office; no immunologic studies in patient and donor
samples were performed.
Transfusion-related risk factors.
Among 71 patients with PPH, 20 (28% ) were transfused with only RBC, 44
(62%) with RBC and FFP and 7 (10%) with RBC, FFP and PLT. Overall, the
number of patients receiving all the three blood products was higher in
the TRALI than in no-TRALI group (p=0,025, Table 1). As shown in Table 1, patients with TRALI received a higher number of units of RBC (p=0,008), PLT (p=0,008) and FFP (p=0,034). Overall, patients in the TRALI group received a higher number of blood products from female donors (p=0,047, Table 1).
RBC and PLT units transfused to patient with or without TRALI had
similar storage times and patients in the TRALI group did not receive
higher number of "old" RBC units (i.e. those units stored for more than
14 days) (Table 1).
Patient-related risk factors. The clinical features of patients grouped according to the diagnosis of TRALI are shown in Table 2.
TRALI was not associated to age or smoking. Pre-existing diseases were
recorded in 21 (30 %) patients and included: hypothyroidism (5),
obesity (4), heart valvular diseases (2), HCV hepatitis (2), asthma
(1), HIV infection (1), Poland syndrome (1 pt) , sickle cell disease
(1), Marfan syndrome (1 pt), hyperthyroidism (1), type I (1) and type
II diabetes mellitus(1), HBV hepatitis (1), liver failure due to
Crigler-Najjar disease (1), systemic lupus erythematosus (1); 3
patients had more than one disease. Among patients with pre-existing
diseases, seven experienced TRALI (50%) and 14 did not (24%) (p=0.099, Table 2).
TRALI did not occur in the two patients with heart valvular disease,
whereas one of them had TACO. Non-hypertensive co-morbidities related
to pregnancy occurred in 7 patients and included anemia (2),
gestational diabetes (2), hypothyroidism (2) and intra-hepatic
cholestasis (1), in similar proportions between TRALI and no-TRALI
groups (Table 2). Eight
patients had pregnancy-related hypertensive disorders: 4 suffered from
gestational hypertension, 2 were affected by gestational hypertension
with superimposed pre-eclampsia, and two patients had pre-eclampsia.[18] Overall, 5 of them experienced TRALI (Table 2). Indeed, hypertensive disorders were overrepresented among patients with TRALI/possible TRALI (36% versus 5%, p=0.006, Table 2).
In contrast, patients with and without TRALI had similar obstetric
issues, including parity, vaginal or cesarean section delivery, number
of previous pregnancies, estimated blood losses and necessity of
surgical intervention (Table 2).
In addition, other acknowledged risk factors for PPH such as uterine
atony, previous uterine surgery, oxytocin administration or placental
abnormalities were equally represented among patients with or without
TRALI (data not shown). Finally, patients with TRALI were more
frequently admitted to the ICU and had a longer hospitalization (p=0.021 and p<0.0001, respectively, Table 2).
Analysis of combined risk factors.
We next examined the concomitant effect of transfusion- and
patient-related factors on the risk to develop TRALI, by combining in a
multivariate model all factors that in univariate analysis had a
significance level of 10% (p < 0.1, Table 3).
We found that only pregnancy-related hypertensive disorders were
significant predictors for TRALI, with an OR of 27.7 (95% CI
1.27-604.3, p=0.034) (Table 3).
In order to ascertain if these underlying conditions were not merely
increasing the risk of transfusion rather than risk of TRALI, we
compared the amount of RBC, FFP and PLT transfused to patients with and
without hypertensive disorders. We found that patients with
hypertensive disorders required similar amounts of blood products as
patients without hypertensive disorders (p=0.699 for RBC, p=0.685 for FFP and p=0.325
for PLT, respectively), suggesting that the higher risk for TRALI
observed in these patients is not dependent on blood volume transfused.
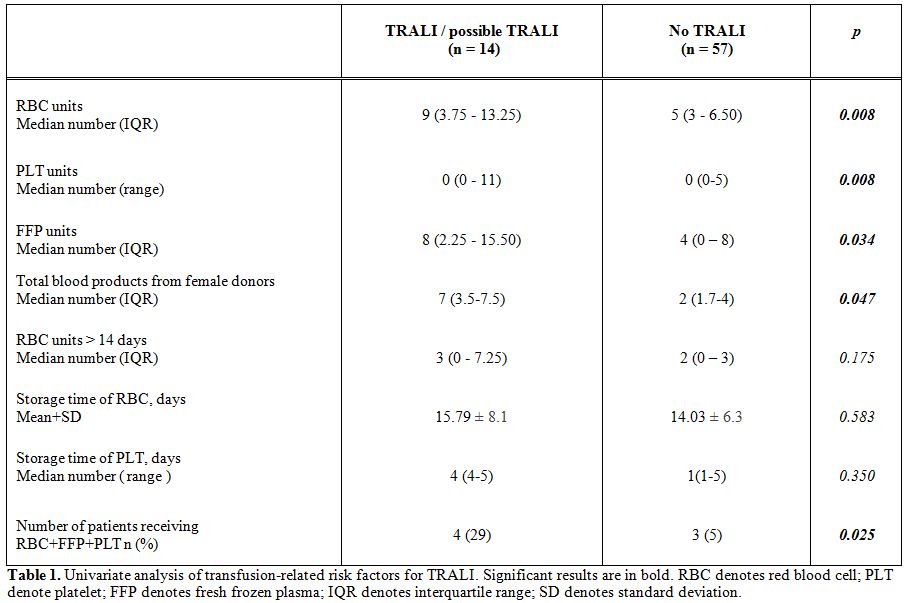 |
Table 1. Univariate analysis of transfusion-related risk factors for TRALI. Significant results are in bold. RBC denotes red blood cell; PLT denote platelet; FFP denotes fresh frozen plasma; IQR denotes interquartile range; SD denotes standard deviation |
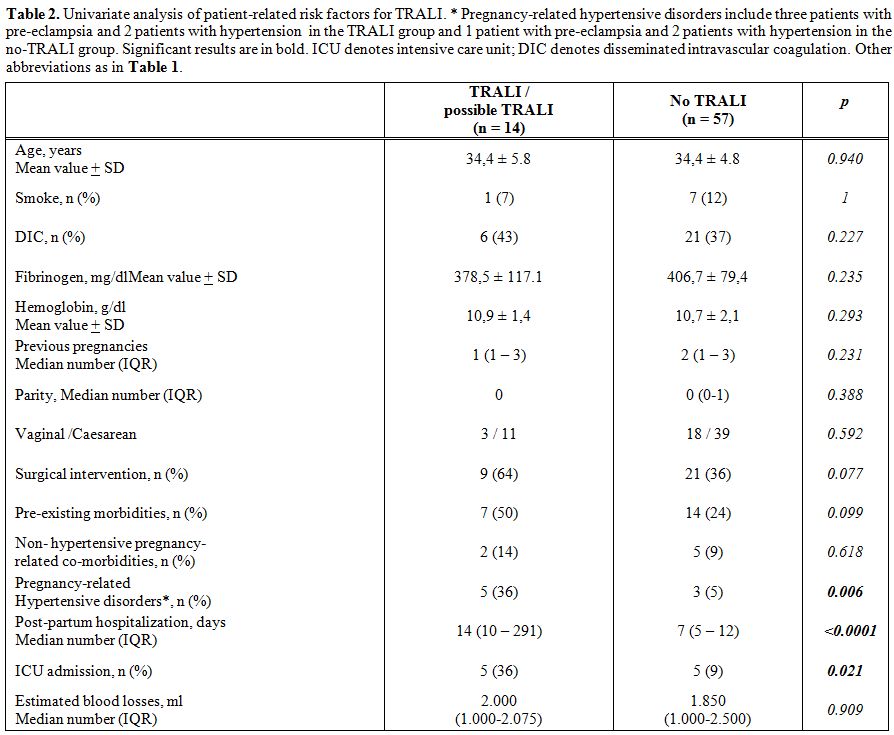 |
Table 2. Univariate analysis of patient-related risk factors for TRALI. * Pregnancy-related hypertensive disorders include three patients with pre-eclampsia and 2 patients with hypertension in the TRALI group and 1 patient with pre-eclampsia and 2 patients with hypertension in the no-TRALI group. Significant results are in bold. ICU denotes intensive care unit; DIC denotes disseminated intravascular coagulation. Other abbreviations as in Table 1. |
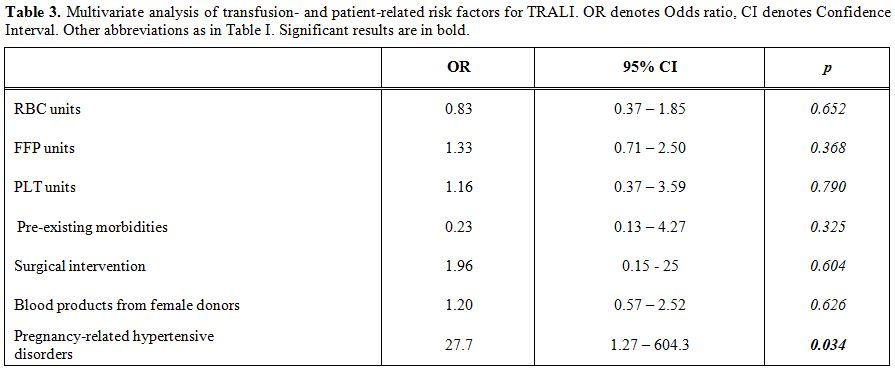 |
Table 3. Multivariate analysis of transfusion- and patient-related risk factors for TRALI. OR denotes Odds ratio, CI denotes Confidence Interval. Other abbreviations as in Table I. Significant results are in bold. |
Discussion
Previous hemovigilance studies suggest that 6.7 to 15% of reported TRALI occur among obstetrics-gynecological patients,[19,20] but data so far published within in this setting are scarce or even anecdotal.[21,22]
In our retrospective series of heavily transfused patients, we found an
overall incidence of TRALI/ pTRALI of 16,9%, that is noteworthy. We
investigated a limited number of patients, representing a fraction of
the overall population with PPH admitted to our hospital in the same
period. Nonetheless, our study is the first attempt to identify TRALI
incidence and risk factors in the obstetrics-gynecology population. In
general, critically ill patients have the highest risk to develop
TRALI, with reported incidence ranging from 1,8 to 15%.[5]
In PPH patients, as well as in general people, the amounts of
transfused products constitute a predictable risk factor for TRALI,
with a significant increase of risk in patients receiving all three
types of blood components. In order to reduce the TRALI risk, female
donors with previous pregnancies or miscarriages as well as donors who
had been previously transfused, are currently no longer eligible for
plasma donations in many countries.[19,23]
Since this policy started in Italy only in mid-2011, many patients
included in this study had probably received antibody-positive blood
products. Accordingly, also in our series we found a possible
implication of blood products from female donors in inducing TRALI. In
addition, our findings suggest that in the obstetric setting the
predisposition to TRALI is also driven by clinical condition of
patients. We found that pregnancy-related hypertensive disorders,
encompassing gestational hypertension and pre-eclampsia, are the most
significant predictors for TRALI, with an increase of risk for
developing this complication of about 27 folds. Severe hypertension
with pulmonary edema can frequently complicate preeclampsia;[18,24,25]
therefore, in pre-eclamptic patients, a careful differential diagnosis
with this condition is mandatory. In particular, among our patients
with pre-eclampsia, three developed the hypoxemia. In these patients,
hypoxemia was not associated with severe hypertension and was not
responsive to diuretic administration, suggesting that an underlying
cause different from pulmonary edema. Several recent studies
demonstrated that various cell types can act as multipliers or
attenuators of TRALI, including platelets,[26] monocytes and T lymphocytes,[27] and endothelial cells themselves.[28]
Clinical manifestations of pregnancy-related hypertensive disorders
reflect a widespread endothelial cell dysfunction, likely due to the
release of soluble factors from the ischemic placenta.[24,25]
Recently, Caudrillier et al. reported that targeting platelet
activation with either aspirin or a glycoprotein IIb/IIIa inhibitor, is
also able to protects mice in an experimental TRALI model.[26]
Therefore, even though our multivariate analysis relies on a low number
of TRALI patients, the mechanisms underlying pregnancy-related
hypertensive disorders support our findings. In fact, a hypothetical
platelet-mediated mechanism could underlie pulmonary endothelial
breakdown in TRALI and organ vascular damage in pre-eclampsia. Notably,
none among our hypertensive patients developing TRALI assumed
antiplatelet agents at the time of delivery. Moreover, TRALI occurred
in all the three hypertensive patients who did not receive
anti-hypertensive therapy but only in two out of five patients
receiving alpha-methyldopa, thus suggesting that a tight control of
hypertension may help to mitigate the TRALI risk.
The main
limitation of our study is the lack of an immunologic confirmatory test
in TRALI cases, aimed to detect the antibody-mediated nature of lung
injury.[6] From a clinical point of view, several
pre-existing conditions (such as neurologic or valvular heart diseases)
or new occurring diseases (such as infections, inhalation of gastric
content during general anesthesia, amniotic fluid embolism) can cause
respiratory distress during post-partum.[2] The
revision of clinical records allowed us to detect or to rule out
frequent causes of ALI, like pneumonia, aspiration or sepsis.[6]
About amniotic fluid embolism (AFE), the reported incidence is very
low, ranging from 1.9 to 6,1 cases per 100,000 maternities.[29]
Accordingly, among 22,344 deliveries occurred at our hospital in the
same period of the study, no cases of AFE were observed. Finally, we
could reasonably rule out TACO in our TRALI patients. TACO, usually,
occurs in elderly people with poor cardiovascular function, often after
FFP transfusion to reverse anticoagulation.[17] Importantly, respiratory distress due to TACO rapidly improves with diuretic therapy.[17]
In contrast, in our patients with TRALI, the respiratory distress was
not ameliorated by diuretic administration, suggesting that the
pulmonary edema not be caused by cardiac dysfunctions or elevated
systemic vascular resistance. Finally, we would emphasize that all
patients included in the study were subjected to continuous monitoring
of ECG, p02, blood pressure and breath rate in the delivery room. This
procedure allowed the prompt detection of hypoxia and facilitated to
define the timing of hypoxia onset in respect to transfusion.
Conclusion
Our findings suggest that patients undergoing massive transfusion in post-partum are highly predisposed to develop TRALI: these observations can be particularly relevant in those countries where female donors with previous pregnancies or miscarriages as well as donors who had been previously transfused are still eligible for plasma donations. The strong association between pregnancy-related hypertensive disorders and TRALI predisposition deserves to be confirmed in a prospective evaluation. Moreover, future studies could definitely ascertain if therapies to treat hypertension and prevent pre-eclampsia also reduce the TRALI risk. In the meanwhile, the close observation of patients suffering from hypertensive disorders after transfusion should be recommended.
Author’s Contribution
References

[TOP]