Received: August 22, 2014
Accepted: November 14, 2014
Mediterr J Hematol Infect Dis 2015, 7(1): e2015002, DOI 10.4084/MJHID.2015.002
This article is available on PDF format at:

Abraham Tareq Yacoub1, Dani Thomas2, Carol Yuan2, Carolina Collazo3, John Greene2, Frank Walsh2, David Solomon2, Skai Schwartz3 and Arthur Andrews4
1 Moffitt Cancer Center, 12902 Magnolia Drive. Tampa, Florida 33612-9497
2 University of South Florida. Morsani College of Medicine. Moffitt Cancer Center
3 University of South Florida
4
James A. Haley Veterans Administration Hospital. University of South
Florida. Morsani College of Medicine. Moffitt Cancer Center
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract There is significant morbidity and
mortality from pneumonia in leukemic and bone marrow transplant
patients. We sought to explore the diagnostic yield of bronchoalveolar
lavage (BAL) in these patients with new pulmonary infiltrates. A
retrospective chart review of approximately 200 Non-human
immunodeficiency virus (HIV) leukemic and Hematopoietic stem cell
transplantation (HSCT) patients who underwent bronchoscopy at a single
academic cancer center was performed. Antimicrobial use for less than
24 hours at the time of BAL was associated with a higher yield in this
population (56.8% versus 32.8%, p<0.001). This supports performing
bronchoscopy with BAL within 24 hours of antimicrobial therapy in
leukemic and HSCT patients. |
Introduction
Pneumonia carries significant morbidity and mortality in leukemic and bone marrow transplant patients.[1,2] The development of pulmonary infiltrates in the setting of such immunocompromise raises concern for both infectious and non-infectious etiologies, some of which are potentially treatable. Many of these patients are receiving broad-spectrum antimicrobials when they develop the infiltrates, either for prophylactic or treatment purposes. The use of bronchoscopy as a diagnostic tool in these immunocompromised patients with lung infiltrates has been well described and is common in clinical practice.[3,4] Performing bronchoscopy provides several different options for sampling the lower respiratory tract. Among these, bronchoalveolar lavage (BAL) is especially effective at collecting samples from the alveoli and has been shown to be associated with less risk than transbonchial biopsy.[4,5] Indeed, BAL has been documented as a diagnostic tool for identifying causative pathogens as well as non infectious etiologies in immunocompromised populations[3] and is common clinical practice. The reported diagnostic yield of BAL in immunocompromised patients, including those with HIV or solid organ transplant, with pulmonary infiltrates ranges widely from 22 to 80%.[5-9] Studies of BAL sensitivity in hematopoietic stem cell transplant (HSCT) patients report yields of 22-65%.[6,7,9-12] With respect to the yield of BAL in non-resolving pneumonia one study in the general intensive care unit (ICU) setting, Pereira Gomes reported a 72% yield in 53 patients.[13] We sought to examine the effect of antimicrobial treatment on BAL results in a large study population of leukemic and bone marrow transplant patients.
Subjects and Methods
This retrospective chart review was performed at a single academic
cancer center. A power analysis was performed to determine the
appropriate sample size. Estimating from the literature specific to our
population[6,7,9,11,12,14-16] we calculated a sample size of 300 with a
power of 0.8 to detect an increase in BAL yield of 23% if the BAL was
obtained within 24 hours of antibiotic use. The patients were selected
from those who had undergone an inpatient bronchoscopy in reverse
chronological order until 300 patients with either a hematopoietic stem
cell transplant or hematologic malignancy were identified. The
exclusion criteria were age <18, a diagnosis of HIV or acquired
immune deficiency syndrome (AIDS), or outpatient status. Electronic
medical records were reviewed and data extracted by a single
investigator, CY. Data including age, sex, cancer diagnosis, time from
HSCT, leukocyte count, neutropenia in addition to medications were
collected. A normal white blood cell (WBC) count was considered
4,000-12,000/mm3. Neutropenia was defined as an absolute neutrophil count (ANC) less than 500/mm3.
Medications including antibiotic duration and timing, antifungal use,
immunosuppressant use or glucocorticoids were recorded. Glucocorticoids
were converted to prednisone equivalents and were documented if the
patient had received at least 20mg daily for > 2 months or 60mg
daily for > 3 weeks. A positive BAL yield was defined as the culture
identification of at least one organism known to be pathogenic in this
patient population. Candida species and coagulase negative staphylocci
were considered colonizers. Our infectious disease expert, JG,
clarified discrepancies. The bronchoscopy technique and procedure was
similar for each patient, utilizing a Fujinon 470S bronchoscope for
every procedure, with the same systematic methodology, as is the
routine at this academic cancer center. Each bronchoscopy was performed
by an attending physician or by a pulmonary fellow with direct
attending supervision. The BAL specimens were collected without suction
connected to the bronchoscope prior to a systematic airway survey. The
BAL was performed by instilling two 60cc aliquots of room temperature
sterile 0.9% saline followed by slow manual aspiration. The specific
subsegmental bronchus from which the BAL specimens were obtained was
recorded. In addition, the volume yield and color of each specimen were
documented in most cases.
Correlates of a positive BAL yield and
time on antibiotics were initially analyzed via a chi-square test, or a
Fisher’s exact test if the expected count was less than 5. Assuming a
binomial distribution, a log-risk model was employed to estimate the
risk ratio of a positive yield with respect to antibiotic duration less
than 24 hours. An adjusted risk ratio was estimated by adjusting this
model for the factors found to be associated with a positive BAL yield
and time on antibiotics. Statistical analyses were performed with
Statistical Analysis Software Version 9.3.
Results
A total of 302 patient records were evaluated. Three patient records
were lacking BAL data. Two patient records were lacking data about
antimicrobial therapy. These patients were therefore excluded from
antibiotic related statistical analyses, leaving a total of 297
patients. All but 5 patients were on antifungal therapy. One patient
had insufficient data about antibiotic duration, and one lacked
adequate medication data.
The age range was 18-85 with an average
age of 53.5. Thirty eight percent of the patients were female and 41.8%
of the patients had undergone HSCT. A minority of the patients required
mechanical ventilation either at the time of BAL or within 48 hours.
These demographic data are presented in Table 1.
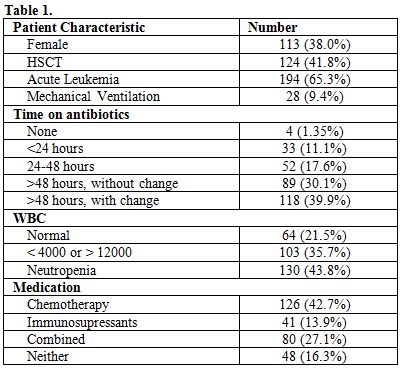 |
Table 1. |
One hundred seven of the 297 patients had a positive BAL culture for an overall BAL yield of 36%. There was not a statistically significant difference between the overall incidence of a positive BAL yield and antibiotic duration. There was a significant association when the patients were stratified according to a 24-hour timeframe. Of the 37 patients on antibiotics for less than 24 hours, including all 4 patients who were not on any antibiotics, twenty-one (56.8%) had a positive BAL culture compared with eighty-five of the 259 (32.8%) patients who had been on antibiotics longer than 24 hours at the time the BAL specimen was obtained and had a positive culture, (p<0.001). Among patients who were on antibiotics for 24 to 48 hours or >48 hours at the time of BAL, the yields were essentially the same at 30.8% and 30.3%, respectively. Among the patients who were on antibiotics for more than 48 hours, 118 of them had their antibiotic regimen changed within 48 hours of their BAL. The BAL culture was positive in 42 (35.6%) of these patients. There were 27/89 (30.3%) patients on antibiotics for more than 48 hours who did not have their regimen changed within 48 hours of their positive BAL. These data are presented in Table 2.
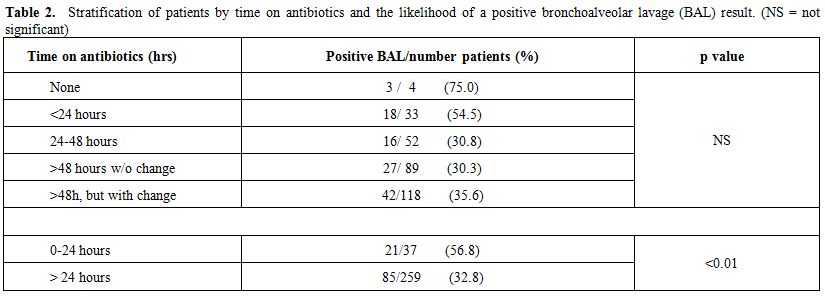 |
Table 2. Stratification of patients by time on antibiotics and the likelihood of a positive bronchoalveolar lavage (BAL) result. (NS = not significant) |
Forty-eight
patients were not receiving chemotherapy or immunosupressants, 15
(31.3%) of whom had a positive BAL yield. One hundred twenty-six
patients were on chemotherapy and 32 (25.4%) had a positive BAL
culture. Forty-one patients were not on chemotherapy but were on
immunosupressants and 14 (34.1%) had a positive BAL yield. Eighty
patients were on both chemotherapy and immunosupressants and 46 (57.5%)
had a positive BAL culture. This is illustrated in Table 3.
We
evaluated leukocyte count and neutropenia with respect to BAL yield.
There were 64 patients with a normal WBC count and 30 (46.9%) had a
positive BAL culture. Patients with an abnormal WBC or frank
neutropenia were less likely to have a positive BAL yield with 39.8%
and 27.7% positive yield, respectively.
Whether the patient was on
a ventilator was also evaluated. There were 23 patients on mechanical
ventilation at the time of their BAL and 12 (52.2%) had positive
cultures. 90 of 269 (33.5%) patients who were not mechanically
ventilated had a positive BAL. This is depicted in Table 3.
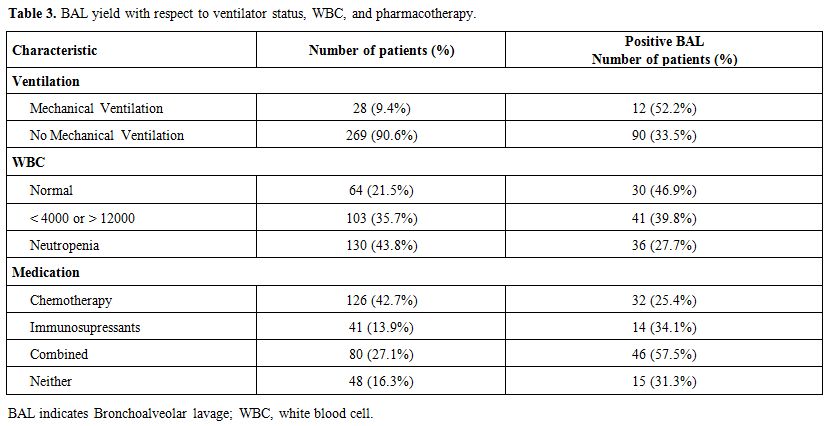 |
Table 3. BAL yield with respect to ventilator status, WBC, and pharmacotherapy. |
Prior to dichotomizing the duration of antibiotics, the association of antibiotic duration with a positive BAL yield was not statistically significant. Table 4 compares patients who were on antibiotics for at least 24 hours prior to obtaining the BAL specimen to those who were on antimicrobials less than 24 hours before the procedure. Patients who were on antibiotics for at least 24 hours were significantly less likely to have a positive BAL yield (32.8% vs. 56.8%, p<0.01). They were also more likely to have leukemia, an abnormal WBC count, and less likely to be on a combination of chemotherapy and immunosupressants together. The risk ratio for a positive yield adjusted for leukemia, abnormal WBC count, and concurrent chemotherapy with immunosuppressant agents was 0.734 (95%CI 0.519-1.037, p=0.078).
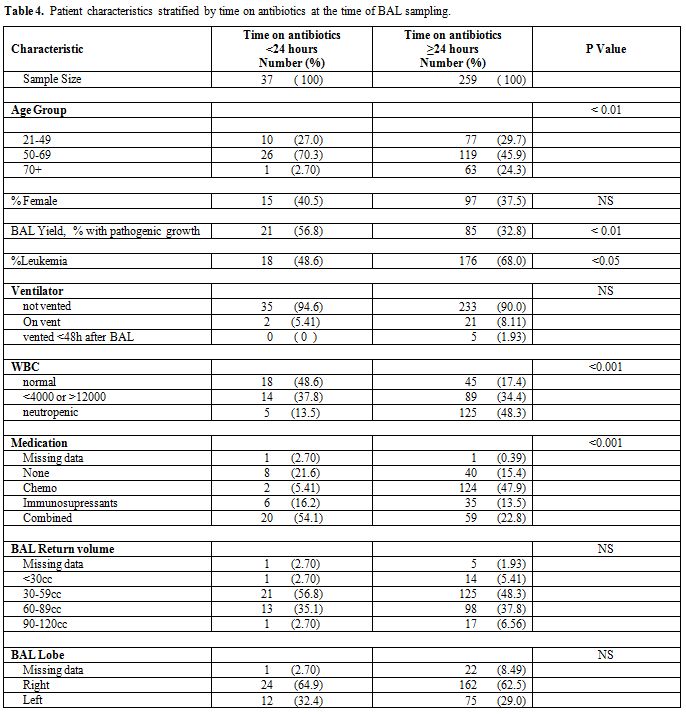 |
Table 4. Patient characteristics stratified by time on antibiotics at the time of BAL sampling. |
There were no statistically
significant differences in the BAL effluent color, volume, or whether
it originated from the right or left lung with respect to incidence of
positive BAL yield.
Among the positive yields, there was no
significant difference in overall distribution of pathogen type. There
was a non-significant trend toward a lower incidence of fungi in those
on antibiotics for at least 24 hours. (Tables 5, 6 and 7)
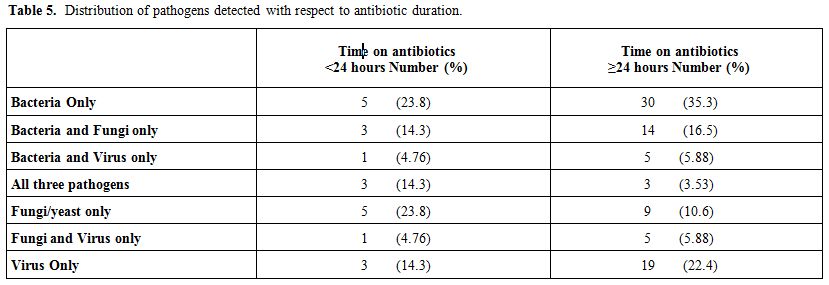 |
Table 5. Distribution of pathogens detected with respect to antibiotic duration. |
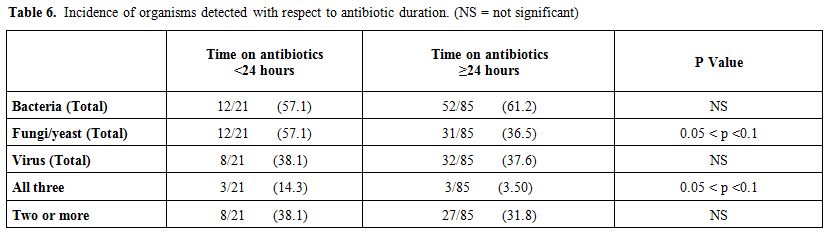 |
Table 6. Incidence of organisms detected with respect to antibiotic duration. (NS = not significant) |
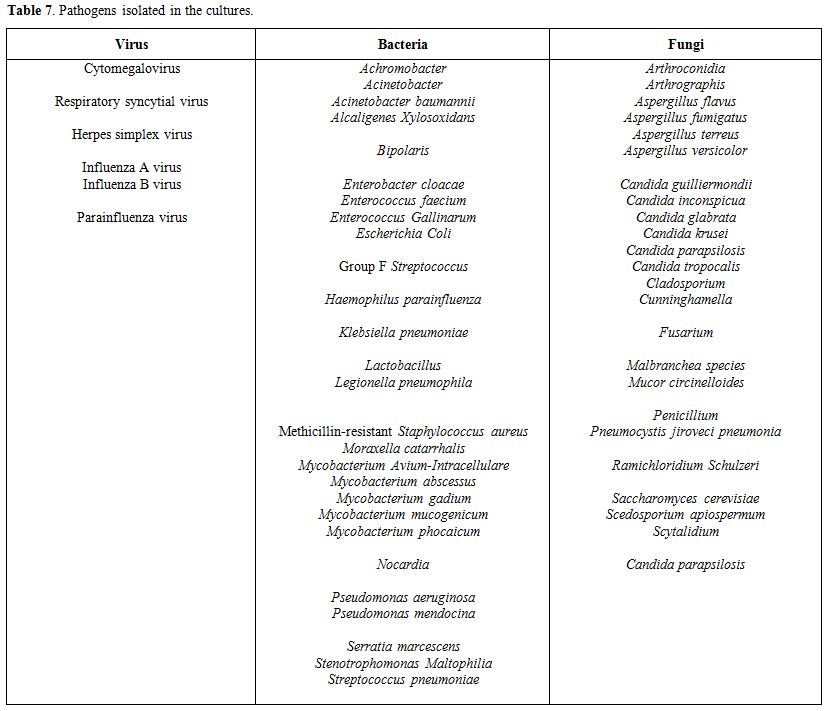 |
Table 7. Pathogens isolated in the cultures. |
Discussion
Acknowledgments
The authors would like to thank the University of South Florida and Moffitt Cancer Center.
References
 . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . [TOP]