Received: September 2, 2014
Accepted: January 8, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015014, DOI 10.4084/MJHID.2015.014
This article is available on PDF format at:

Hacettepe University, Faculty of Medicine, Department of Hematology, Ankara, Turkey.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract The aim of this paper is to outline
pharmacotherapy of the ‘third-line management of CML’ (progressive
disease course after sequential TKI drugs). Current management of CML
with multi-TKI failure is reviewed. TKI (bosutinib, ponatinib,
dasatinib, nilotinib) and non-TKI (omacetaxine mepussecinate, IFN or
PEG-IFN) drugs are available. The literature search was made in PubMed
with particular focus on the clinical trials, recommendations,
guidelines and expert opinions, as well as international
recommendations. Progressing CML disease with multi-TKI failure should
be treated with alloSCT based on the availability of the donor and EBMT
transplant risk scores. The TKI and non-TKI drugs shall be used to get
best promising (hematological, cytogenetic, molecular) response. During
the CP-CML phase of multi-TKI failure, 2nd generation TKIs (nilotinib
or dasatinib) should be tried if not previously utilized. Bosutinib and
ponatinib (3rd-generation TKIs) should be administered in double- or
triple-TKI (imatinib and nilotinib and dasatinib) resistant patients.
The presence of T315I mutation at any phase requires ponatinib or
omacetaxine mepussecinate therapy before allografting. During the
AP/BC-CML phase of multi-TKI failure, the most powerful TKI available
(ponatinib or dasatinib if not previously used) together with
chemotherapy should be given before alloSCT. Monitoring of CML disease
and drug off-target risks (particularly vascular thrombotic events) are
vital. |
Introduction
Chronic myeloid leukemia (CML) is a slowly progressive clonal
malignant disease characterized by myeloid neoplastic expansion with
heterogeneous clinical manifestations.
Tyrosine kinase
inhibitors (TKIs) therapy induces high rate of response in the majority
of patients. However, while a large proportion of patients attains a
prolonged molecular response, and some of them could be considered
cured, a not negligible number of patients show a
resistance to TKIs therapy.[1] Standardized therapeutic approach may be
useful in the de novo or TKI-responsive patient with CML since TKIs
could successfully modulate the disease course.[2-4] On the contrary,
the treatment schedule should be personalized in the CML patient with
progressive disease, despite the administrations of more than one TKI
(multi-TKIs).[1]
Disease progression under TKIs is a ‘difficult-to-treat’ situation with the available drugs in CML.[5]
The
aim of this paper is to outline the perspectives for the drug therapy
choices in the CML patient with progressive disease course after
sequential multi-TKIs regimen. This clinical approach is known as
‘third-line management of CML’ in the current TKIs era.
CML Disease Status and Challenges after multi-TKI Failure
The decision for the choice
of TKIs drug depends upon the best available evidence obtained from
randomized clinical trials (RCT), physician experience, and
characteristics of the patient and his/her disease. In the “real
world”, the management of resistant CML should have an integrative
approach including: drug (efficacy, safety, tolerability,
toxicity, and pharmacoeconomic of the TKI), the patient (CML disease
risk, age, co-morbidities, molecular BCR-ABL dynamics, compliance,
lifestyle, adherence, drug off-target risk profile), and the status of
local medical assistance (TKI availability, TKI reimbursability, drug/
disease experience of physician, CML monitoring techniques, the
cooperation between CML specialized centre and the home doctors).[1]
Most of those critical parameters are negatively affected in the CML
patient with progressive disease course after sequential multi-TKI
regimen. TKIs have been investigated in RCT mostly in the newly
diagnosed, de novo, first-line patients. Clinical investigations, made
in the CML patients where imatinib failed, are mostly open-label,
non-comparative trials. Furthermore, the sequential use of 2nd
generation TKIs (nilotinib and dasatinib, one after the other) had not
been studied in well-designed proper prospective randomized clinical
trials.
Disease duration is important in the pathobiology of CML. Figure 1
illustrates that time is matter in CML. As a function of time, Ph*(+)
neoplastic hematopoiesis dominates blood cell production at onset of
the disease. Over time, self-renewal of leukemic CML stem cells,
genomic instability, impaired DNA repair mechanisms,
proliferation/anti-apoptosis of Ph*(+) neoplastic progenitors, clonal
selection, and the acquisition of additional mutagenic events do
complicate the biology of CML, as well as the clinical manifestations.
Moreover, the oxidative stress, increased by BCR-ABL tyrosine
kinase, and the altered mutational phenotype further accelerate
the disease course.[5]
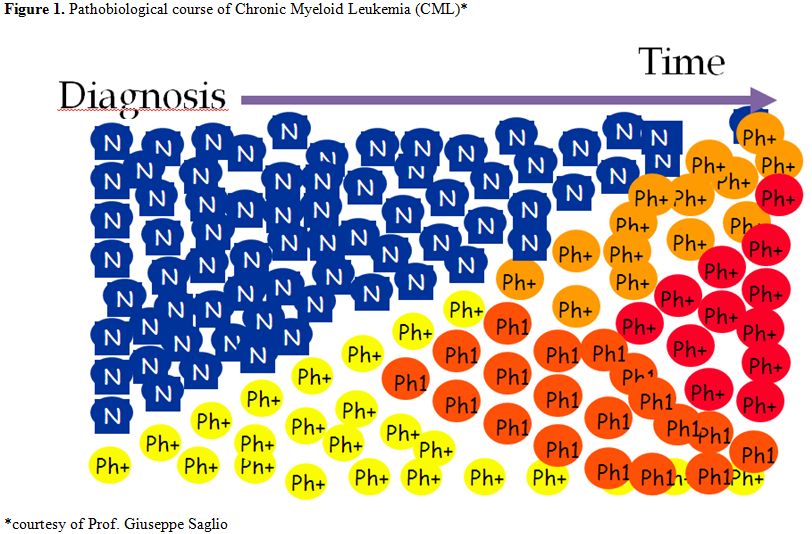 |
Figure 1. Pathobiological course of Chronic Myeloid Leukemia (CML) [courtesy of Prof. Giuseppe Saglio] |
Terminal stage of this malignant neoplastic
development is the accelerated phase (AP)/ blastic crisis (BC) of CML.
Late progressing chronic phase (CP), uncontrolled under TKIs, is also a
precarious situation prone to AP/BC CML. The terrible end of CML makes
‘prevention of disease progression’ is the ultimate aim of TKI
treatment. Thus, early and rapid reduction of BCR-ABL with acceptable
TKIs control is a primary goal of CML therapy. Of course, this goal had
already failed in the CML patients with progressive disease after the
intake of sequential multi-TKI regimens.[2] Most importantly, after
each additional failed treatment line, the probability of developing
new mutations (including compound mutations that confer high-level
resistance to TKI therapy) and CML progression enhance.
How to Proceed to Manage CML Disease after multi-TKI Failure?
European LeukemiaNet (ELN) recommendations
indicated the way of management in the de novo or TKI-responsive CML
patient, based on the data obtained from numerous RCTs.[2]
However, the level of evidence is low for decision making about the
choice of drugs in the CML patient resistant to previous multi-TKI
drugs. Official ELN recommendation for third-line CML treatment
(failure of and/or intolerance to 2 TKIs) in CP-phase is “..Anyone
of the remaining TKIs; allogeneic hematopoietic stem cell
transplantation (alloSCT) recommended in all eligible patients (HLA
type patients and siblings; search for an unrelated stem cell donor;
consider alloSCT)” quite similar to the suggestions in the AP/BC phase-CML “..Anyone
of the TKIs that were not used before progression (ponatinib in case of
T315I mutation), then alloSCT in all patients. Chemotherapy is
frequently required to make patients eligible for alloSCT”.[2]
Several
clinical scenarios (and drug suggestions accordingly) can be generated
to describe the ‘third-line CML’ from the ELN recommendations;
•
The CML patient with failure of imatinib and dasatinib (candidate for
nilotinib, bosutinib, ponatinib; then alloSCT)
•
The CML patient with failure of imatinib and nilotinib (candidate for
dasatinib, bosutinib, ponatinib; then alloSCT)
• The CML patient with failure of nilotinib and dasatinib (candidate for bosutinib, ponatinib; then alloSCT)
• The CML patient with failure of nilotinib and bosutinib (candidate for dasatinib, ponatinib; then alloSCT)
• The CML patient with failure of dasatinib and bosutinib (candidate for nilotinib, ponatinib; then alloSCT)
The timing of alloSCT has changed to third- or fourth-line CML after failure of the second-generation TKIs.[2,6]
The definition of transplant eligibility is never absolute since it is
based on the balance between the disease risk of CML and the
mortality/morbidity risk of alloSCT.[5]
Mutational
analyzes shall be performed in all of the CML cases with multi-TKI
failure during the drug treatment decision. BCR-ABL1 kinase domain
point mutations are detectable in about 50% of patients with treatment
failure and progression. The mutations detected during the TKI therapy
may be resulted in drug switches based on the nature of the mutation.
Dasatinib and nilotinib retain activity against most of the mutations
that confer resistance to imatinib. Likewise, distinct mutations
exhibit decreased sensitivity to dasatinib versus nilotinib.[7]
T315I, Y253K, E255K, E255V, F359V, F359C, are the mutations poorly
sensitive to nilotinib; whereas T315I, T315A, F317L, F317C, V299L are
the mutations poorly sensitive to dasatinib. There is also an extensive
evidence that Bosutinib al has activity against most of the mutations
that confer resistance to imatinib. Bosutinib also showed activity
against Nilotinib resistant mutations including Y253H, E255K/V and
F359C/V and Dasatinib resistant mutations including F317C and E255K/V.
T315I is a unique mutation making the CML patient irresponsive to all
available TKIs but ponatinib, non-TKI drug omacetaxine mepussecinate
and allografting.[7] In the CML patients with the
T315I mutation, where effective treatment options are limited,
ponatinib continued to exhibit deep and durable responses with up to 6
years follow-up. Dose reductions, to manage adverse events, did not
impact maintenance of cytogenetic response. The response rate and
safety profile of T315I patients were comparable to those observed in
the overall population of refractory CML and Ph+, ALL patients in
ponatinib clinical trials.[8] No mutation conferring resistance to Ponatinib, so far, has been identified.[2,9,10]
With longer follow-up and the availability of second and third
generation TKIs, most clinically relevant ABL kinase mutations respond
to change in TKI therapy following imatinib failure, with the majority
of patients achieving durable cytogenetic and molecular responses. An
early detection and characterization of ABL kinase mutations shall be
performed in imatinib-resistant patients in order to identify the
patients who may benefit from alternative TKI therapy or stem cell
transplantation. In the Palani study,[11]
eighty-three ABL kinase mutations were detected in 65 CP-CML patients
at the time of imatinib failure with 35% of patients (23 of 65)
harboring P-loop mutations (including M244V), 18% (12 of 65) with T315I
mutation and 46% (30 of 65) with other mutations (catalytic domain,
imatinib binding site, activation loop and C-terminal). Composite
mutations were present in 10 patients (15%), with two patients
harboring both P-loop and T315I mutations.[11]
Difficulties in the Treatment of CML after multi-TKI Failure
The most challenging situations are failure to
all available TKIs in the patients CML which cannot be transplanted or
relapsing after allografting. These patients need effective and safer
treatment options. Therefore, patient-centered clinical decision is
necessary in this difficult situation.[5] Table 1
summarizes the current status of ‘third-line management of CML’ with
the available drugs. Before the introduction of bosutinib and
ponatinib, CP-CML patients who had failed 2 prior lines of TKI had
limited treatment options with poor treatment response and outcome.
These newer TKIs are important additions to the treatment
armamentarium, but the optimal choice of 3rd-line CML treatment has not been established.[12]
Bosutinib is an oral dual Src/Abl TKI drug. It is recommended in 2nd, 3rd and later lines of CML treatment in both ELN and NCCN guidelines, where appropriate.[2] This is based on the large 2nd line bosutinib study and 3rd
line study with 119 patients – only a few patients were “triple TKI
failed” patients. In this last study, the CML patients (n=119) were
aged ≥18 y, with prior imatinib failure plus dasatinib resistance
(n=38) or intolerance (n=50), nilotinib resistance (n=26), or nilotinib
intolerance or dasatinib resistance/intolerance + nilotinib resistance
/ intolerance (n=5) and received bosutinib starting at 500 mg/day.[13]
Major cytogenetic response (MCyR) was newly attained or maintained from
baseline by 33% and 7% of patients, respectively (32%
attained/maintained complete cytogenetic response [CCyR]). Kaplan-Meier
probability of maintaining MCyR or CCyR at four y was 69% and 54%,
respectively. The most common adverse event with bosutinib was diarrhea
(n=98).[13] Therefore, to suggest that Bosutinib can
only be administered in triple TKIs failed patients after imatinib,
nilotinib and dasatinib does not reflect the wealth of the data nor the
recommendations. This also fits with the patient centred approach[1] which suggests that based on co-morbidities, disease risk, and mutations. The choice in 3rd
line can be from among nilotinib, dasatinib, bosutinib and ponatinib
rather than stipulating the order that they must be used. Bosutinib
could be an option for the CML situations which preclude the use of
other TKIs.[14] In a Spanish study, cross intolerance
with bosutinib was extremely rare, of the 7 patients who had rash with
imatinib, only 1 suffered rash with bosutinib. None of the patients had
pleural effusion with bosutinib out of 15 who previously experience it
with dasatinib neither vascular events out of the ten patients that
already had this side effect with nilotinib. Therefore, in heavily
pretreated CML patients, most of them in 4th-line,
bosutinib had an acceptable safety with no CML patients interrupting
treatment due to side effects also in the previously TKI intolerant
patients. Importantly, the rates of cross intolerance (namely
cardiovascular, pleural and skin) were also very low in the Spanish
study.[14]
Ponatinib is an approved potent oral
TKI active drug against native and the mutant BCR-ABL, including the
resistant T315I mutant. The PACE trial evaluated the efficacy and
safety of ponatinib (45mg qd) in CML and Ph+ ALL patients (n=449)
resistant/intolerant to dasatinib or nilotinib or with the T315I
mutation.[15] Ponatinib is effective in 67% of CP-CML third-line patients. In the PACE Study, 98 patients received ponatinib in 3rd
line (after failure of imatinib and dasatinib or imatinib and
nilotinib. In this subgroup, the response rate (MCyR) was 67%
comparable to that achieved with dasatinib and nilotinib in earlier
treatment lines (second line). In both ELN and NCCN guidelines,
Ponatinib is recommended for use in 3rd line; with the ELN guidelines also indicating ponatinib for use also in 2nd line. Ponatinib is the only single TKI, which has been extensively studied in a large cohort of patients where imatinib and a 2nd
generation TKI have failed. On the contrary, sequential use of
nilotinib and dasatinib in third line has not been studied in
appropriately designed clinical trials and the scarce available
published evidence suggests a scarce efficacy. Garg and co-workers
indicated that the use of second-generation TKI after failure to two
TKIs may induce clinical responses, but those are usually not durable
except in some CP-CML patients.[16] Likewise, bosutinib give a modest benefit in 3rd-line CML[17].
Only 32% of the third-line patients achieved MCyR, and this despite
that close to half (46%) of the patients has not had a problem of
resistance at baseline, but was intolerant to previous TKIS.[17]
The poor efficacy and short duration of response in patients treated
with nilotinib and dasatinib in sequential use, highlight that one
reason for the lack of durable cytogenetic remission could be the
emergence of new kinase domain mutations. Ponatinib could provide a
higher probability of response for patients failing imatinib and
dasatinib/nilotinib compared with sequential 2nd generation TKI therapy commonly used in this indication.[18] In the patients, where one 2nd
generation TKI has failed, the risk of disease progression is high, and
ponatinib, which has demonstrated an unprecedented efficacy in
difficult-to-treat patient population, may be considered as the
therapeutic option, even if it presents an increased risk of thrombotic
vessel occlusions. In fact, in October 2013, PACE trial was placed
on partial clinical hold, due to observation of arterial thrombotic
events in the ponatinib clinical program; following these
events, a dose reduction was recommended. Serious arterial thrombotic
episodes were observed in 19% of the ponatinib-treated patients and
included cardiovascular 10%, cerebrovascular 7%, peripheral vascular 7%
districts. Venous thromboembolic events too were signaled in 5% of the
ponatinib-treated patients. Higher dose-intensity, older age, and
cardiovascular risk factors were associated with higher likelihood of
thrombotic events. However, Ponatinib could exhibit deep and durable
responses in heavily pre-treated patients (58% received ≥3 prior TKIs)
with relatively longer follow-up (median follow-up: 27.9 (0.1-39.5)
months), particularly CP-CML. Initial data suggested that the response
may be maintained after the dose reduction; however, longer follow-up
is needed to understand impact on safety.[15] In the
refractory CML patients, the rapid and profound reduction in BCR-ABL
levels, achieved with Ponatinib, translated into improved long-term
outcomes. The assessing BCR-ABL levels at early time points, as a goal
of therapy with Ponatinib, had been suggested since achieving early
landmark response could be a reliable predictor of better long-term
outcomes.[19] In an ongoing phase 1/2, multi-center,
open-label, dose-finding study of ponatinib in Japanese patients with
CML or Ph+ ALL, who have experienced a failure of dasatinib or
nilotinib therapy, because of resistance or intolerance, ten (59%)
CP-CML patients attained the primary efficacy endpoint of MCyR (6 CCyR,
4 MMR). The primary efficacy endpoint of major hematological response
was achieved by 10 patients: 2/2 AP-CML, 2/4 BP-CML and 6/12 Ph+ ALL
patients. MMR was observed in 5 (14%) CML patients in the Japanese
study.[20] Ponatinib dose intensity is associated
frequently with many adverse side effects. Future investigations (a
dose-ranging trial of ponatinib in refractory CML to evaluate
benefit/risk of different dosing schemes) should focus on lower average
ponatinib dose intensity, such as starting at lower doses and/or
reducing the dose basing on the response level in CML.[21]
Real-world data also indicated that ponatinib is prescribed across
disease phase, therapy line, and mutation status. Physicians have
adopted dose-reduction strategies in both new and especially ongoing
patients; evidence indicates dose-adjustment by age, gender and disease
phase.[22]
Clinical trials in patients who have
failed 2 previous lines of TKI suggest ponatinib may be more
efficacious than bosutinib, but with a less favorable side-effect
profile.[12,17] The comparison of
overall benefit-risk from available clinical trial data is challenging
due to single- arm designs, low overall mortality, disparate impact of
characteristic side-effects, and the likely crossover/sequential use of
alternative TKIs among patients discontinuing therapy.[12]
Levy and coworkers examined the efficacy outcomes, treatment duration
and reason for study drug discontinuation, as surrogates for overall
benefit-risk in 3rd line CP-CML patients treated with ponatinib vs. bosutinib.[12] They used the clinical trial data for bosutinib[17] and PACE for ponatinib[15] for 3rd
line CP-CML. The study examined efficacy outcomes including MCyR, CCyR,
MMR, durability of response, duration on therapy and reasons for
discontinuation among patients treated with ponatinib vs. bosutinib
after failing 2 prior TKIs. In the study, the outcomes were evaluated
at similar follow-up time points: median 28.5 (range 0.3-56.2) months
bosutinib; median 30.5 (0.2-39.8) months ponatinib. The efficacy
outcomes were defined such that patients were required to demonstrate
improvement relative to baseline to be counted as responders.[12]
Their indirect comparison using a variety of surrogate measures
suggested superior efficacy and durability of response with ponatinib
vs. bosutinib in 3rd line CP-CML patients. Based on the results of this indirect comparison, the treatment response was higher for 3rd
line CP-CML patients treated with ponatinib (n=98) than with bosutinib
(n=118) across all measures. MCyR was achieved by 67% of ponatinib vs.
32% of bosutinib patients, CCyR by 56% of ponatinib vs. 24% of
bosutinib patients, and MMR by 42% vs. 15%. The CML patients who
received ponatinib experienced more durable responses with 93% of the
ponatinib patients who achieved MCyR estimated to retain response after
2 years vs. 59% of the bosutinib patients who achieved this response
level. After approximately 2.5 years of follow up, less than one-third
(29%) of bosutinib patients remained on study drug vs. the majority
(57%) of ponatinib patients. The median treatment duration was
substantially shorter for bosutinib vs. ponatinib, with patients
remaining on ponatinib therapy more than 3.5 times as long as on
bosutinib. The majority of 3rd line
bosutinib patients that discontinued did so due to treatment failure
(58.3% of the patients who discontinued), while less than one-quarter
(23.8%) of ponatinib patients who discontinued did so due to failure.[12]
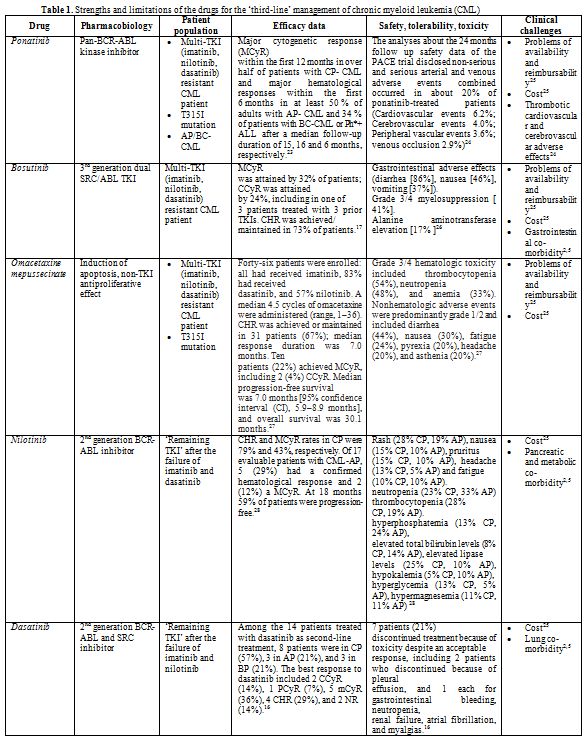 |
Table 1. Strengths and limitations of the drugs for the ‘third-line’ management of chronic myeloid leukemia (CML) |
Perspectives for the Treatment of Progressing CML disease after multi-TKI Failure
Current standard practice is allografting for all of the CML cases with multi-TKI failure based on the availability of the donor and EBMT transplant risk scores. Before the alloSCT, all patients should be treated with the best available ‘remaining’ TKI in order to reach best promising response/ remission land (complete hematological response (CHR), complete cytogenetic response (CCyR), stable molecular response (MR)). For this aim all the drugs “Remaining”, bosutinib, ponatinib, dasatinib, nilotinib, and omacetaxine mepussecinate should be used. During the CP-CML phase of multi-TKI failure, 2nd generation TKIs (nilotinib or dasatinib) are used if remaining. Bosutinib and ponatinib (3rd-generation TKIs) can be administered in double- or triple-TKI failed (Imatinib and nilotinib and dasatinib) patients. The presence of T315I mutation at any phase requires ponatinib or omacetaxine mepussecinate therapy before allografting. Combinations of TKI and interferon (IFN) or PEG-IFN are used in the everyday clinical practice for the unresponsive cases to TKI alone, but limited data is available for the combination approach.[29,30] During the AP/BC -CML phase of multi-TKI failure, the most powerful TKI available (ponatinib or dasatinib if remaining) together with multi-agent chemotherapy[31] should be given before alloSCT.[32] The clinical outcome is more poor for the transplant-ineligible CML patients with multi-TKI failure or post-transplant relapsed patients. TKI (bosutinib, ponatinib, dasatinib, nilotinib) and non-TKI (omacetaxine mepussecinate, IFN or PEG-IFN; including their combinations with TKIs) drugs should be used based on the same principles in those problematic CML patients as summarized above. Monitoring the CML disease and drug off-target risks (particularly vascular thrombotic events) are vital. Expected hematological, cytogenetic, and molecular responses to those drugs during the monitoring of CML are variable, and based on the disease phase, mutational status, resistance profile, age, co-morbidities, molecular BCR-ABL dynamics, compliance, lifestyle, adherence, and drug off-target risk profile.[1] Future candidate CML treatment regimens can be optimized for maximal specificity toward primitive leukemia stem cells.[33]
References

[TOP]