Received: December 21, 2014
Accepted: March 3, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015030, DOI 10.4084/MJHID.2015.030
This article is available on PDF format at:

Abraham T. Yacoub1, Jayasree Krishnan1, Ileana M. Acevedo2, Joseph Halliday2 and John N. Greene1
1 H. Lee Moffitt Cancer Center and Research Institute. 12902 Magnolia Drive. Tampa, Florida 33612-9497.
2
University of South Florida, Morsani College of Medicine, Division of
Infectious Disease and International Medicine, 1 Tampa General Circle,
G323.
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Background. Nutritionally variant Streptococci (NVS), Abiotrophia and Granulicatella
are implicated in causing endocarditis and blood stream infections more
frequently than other sites of infection. Neutropenia and mucositis are
the most common predisposing factors for infection with other pathogens
in cancer patients. In this study, we investigated the clinical
characteristics of NVS bacteremia in cancer patients and identified
risk factors and outcomes associated with these infections. Materials and Methods. We retrospectively reviewed all cases of NVS bacteremia occurring from June 1999 to April 2014 at H. Lee Moffitt Cancer Center and Research Institute. The computerized epidemiology report provided by the microbiology laboratory identified thirteen cancer patients with NVS bacteremia. We collected data regarding baseline demographics and clinical characteristics such as age, sex, underlying malignancy, neutropenic status, duration of neutropenia, treatment, and outcome. Results. Thirteen patients were identified with positive NVS blood stream infection. Ten patients (77%) had hematologic malignancies, including chronic lymphocytic leukemia (CLL) (1), multiple myeloma (MM) (1) acute myelogenous leukemia (AML) (4) and non-Hodgkin’s lymphoma (NHL) (4) The non-hematologic malignancies included esophageal cancer (2) and bladder cancer (1). Conclusion. NVS should be considered as a possible agent of bacteremia in cancer patients with neutropenia and a breach in oral, gastrointestinal and genitourinary mucosa (gingivitis/mucositis). |
Introduction
Nutritionally Variant Streptococci (NVS) (Abiotrophia and Granulicatella) are fastidious Gram-positive bacteria that were described for the first time in 1961.[1] They are also called satelliting streptococci because they usually form satellite colonies around Staphylococcus aureus and other bacteria, including some Enterobacteriaceae and other streptococci.[2] They are a common component of the oral flora but have been associated with a variety of invasive infections.[3] Colonies of NVS are small (0.2 to 0.5 mm in diameter), and are either non-hemolytic or α-hemolytic on blood agar.[4]
The
nutrient requirements of these microbes include cysteine or pyridoxal
(active form of vitamin B6) for growth in complex media.[5,6] NVS are divided in two genera (Abiotrophia and Granulicatella) comprising four species that have been identified from human specimens: Abiotrophia defectiva, Granulicatella adiacens, Granulicatella elegans and Granulicatella para-adiacens.[2]
Materials and methods
We retrospectively reviewed all cases of NVS bacteremia occurring from June 1999 to April 2014 at H. Lee Moffitt Cancer Center and Research Institute. The computerized epidemiology report provided by the microbiology laboratory identified thirteen cancer patients with NVS bacteremia. We collected data regarding baseline demographics and clinical characteristics, such as age, sex, underlying malignancy, neutropenic status, duration of neutropenia, treatment, and outcome. Data was recorded from the Infectious Disease consultation reports and discharge summaries. Resolution of the infection was defined as repeated negative blood cultures. When reporting data, all percentages were rounded to the tenth decimal point.
Results
Thirteen patients were identified with positive NVS blood stream
infection. Ten patients (77%) had hematologic malignancies, including
chronic lymphocytic leukemia (CLL) (1), multiple myeloma (MM) (1),
acute myelogenous leukemia (AML) (4) and non Hodgkin’s lymphoma (NHL)
(4) (Table 1, Figures 1 and 2).
The
non-hematologic malignancies included esophageal cancer (2) and bladder
cancer (1). Seven patients (54%) were neutropenic (defined as Absolute
Neutrophil Count < 1500 cells/uL) with an average duration of 14
days. The median age was 60 years. There was no gender predilection.
Seven patients had mucositis at the time of diagnosis either due to
chemotherapy or graft versus host disease. One patient had gingivitis
with a dental abscess. None of the patients developed infective
endocarditis. Most patients were on empiric antimicrobial therapy with
ciprofloxacin, levofloxacin or piperacillin/tazobactam at the time of
breakthrough bacteremia. Almost all patients received vancomycin as
definitive treatment. All the patients had transient bacteremia with an
average duration of positive blood cultures of 1 day. The 30-day
mortality rate was 16.67%. Mortality was not attributable to NVS
bacteremia
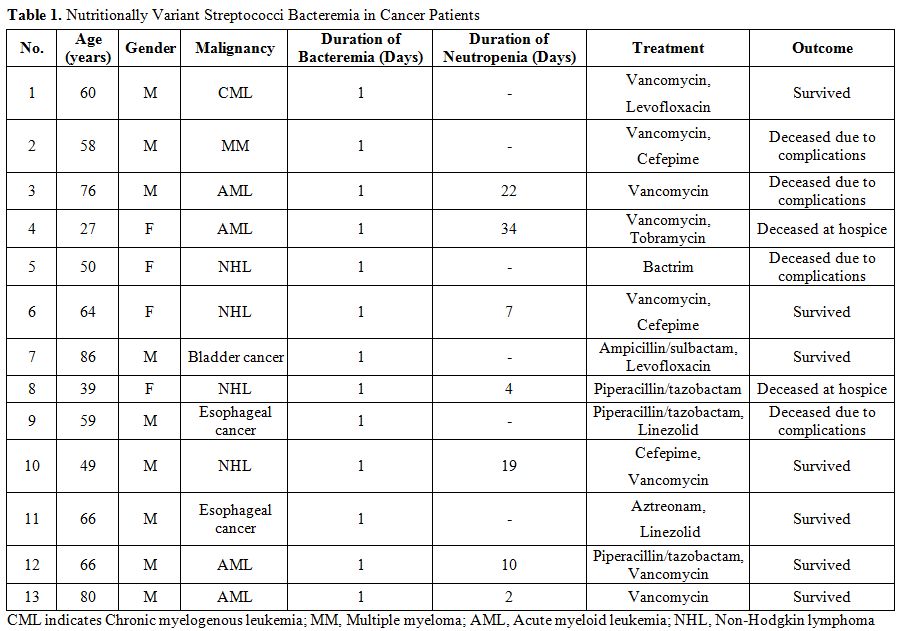 |
Table 1. Nutritionally Variant Streptococci Bacteremia in Cancer Patients |
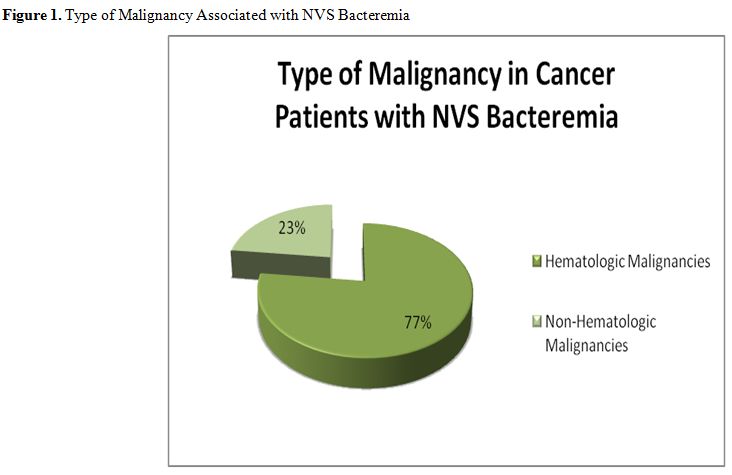 |
Figure 1. Type of Malignancy Associated with NVS Bacteremia |
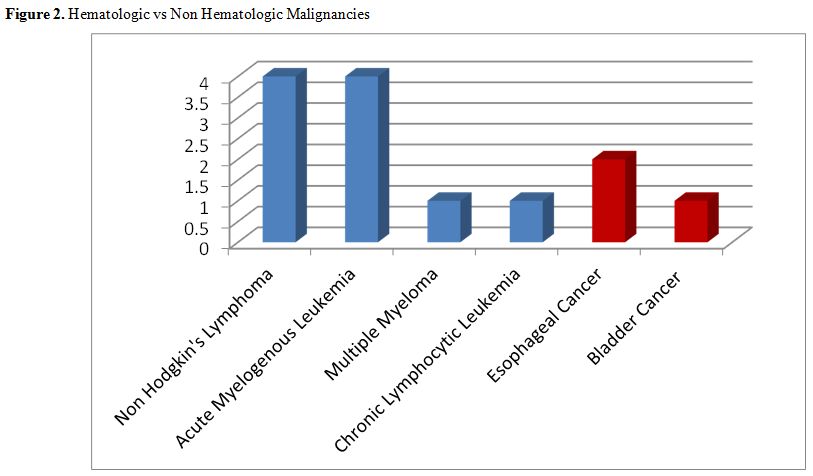 |
Figure 2. Hematologic vs Non Hematologic Malignancies |
Discussion
During this study, we collected the data spanning fourteen years
period (1999-2014) at Moffitt Cancer Center. We found that NVS blood
stream infections are commonly found in hematological malignancies. Our
study was compared to Senn et al, and found that NVS blood stream
infections were common in neutropenic patients with hematological
malignancies.[1]
NVS are typically associated with endocarditis in immunocompetent patients and bacteremia in immunocompromised patients[1,7]
and interestingly none of our patients had developed endocarditis.
Chemotherapy-induced mucositis and neutropenia have previously been
identified as risk factors in cancer patients.[1]
NVS infections have been reported in patients with infectious crystalline keratopathy,[8] vertebral osteomyelitis,[9] endophthalmitis,[10] meningitis[11] and in cancer patients.[12-15]
Once a suspected NVS is cultured, its identity should be confirmed by establishing its requirement for pyridoxal.[2]
This test should be carried out on a medium that is incapable of
supporting the organism's growth without pyridoxal supplementation.[2] A positive pyrrolidonyl arylamidase test along with typical morphology should further serve to identify an isolate as an NVS.[2]
The 16S rRNA gene PCR and restriction fragment length polymorphism
analysis are different modalities to identify different species of NVS.[1,3,16-18]
Endocarditis caused by NVS has a higher rate of complications and treatment failure.[19] NVS blood stream infections should be treated in the same way as viridans streptococci and enterococcus.[3]
It is recommended that a combination therapy of benzyl penicillin and
amoxicillin plus a gentamicin for a course of 4 to 6 weeks is used to
treat these microorganisms.[19,20] Vancomycin is an alternative therapy when a penicillin-aminoglycoside combination is ineffective or contraindicated.[21]
In
our study, most patients were on empiric antimicrobial therapy with
ciprofloxacin, levofloxacin or piperacillin/tazobactam at the time of
breakthrough bacteremia. Almost all patients received vancomycin as
definitive treatment. All the patients had transient bacteremia with an
average duration of positive blood cultures of 1 day.
Unlike
streptococcus viridans, NVS does not typically cause adult respiratory
distress syndrome and septic shock and is more benign.[22,23]
Although patients who develop fungemia, gram-negative bacteremia, or
sepsis syndrome are best treated by catheter removal in addition to
antimicrobial therapy, an increasing body of evidence suggests that
many gram-positive bacterial catheter infections can be treated by use
of antimicrobial agents without catheter removal.[24,25]
Conclusion
NVS should be considered as a possible agent of Gram-positive bacteremia in cancer patients with neutropenia and a breach in oral or gastrointestinal mucosa, especially chemotherapy-induced mucositis or gingivitis. We recommend against routine removal of the central venous catheters given the benign course of NVS bacteremia, rapid clearance from blood, and likely oral or GI tract source of the pathogen. NVS bacteremia did not contribute to the mortality of patients in our study.
References
 ... . ... .. .... . . .... . . . ..
... . ... .. .... . . .... . . . ..[TOP]