Prognostic Value of Brain and Acute Leukemia Cytoplasmic Gene Expression in Egyptian Children with Acute Myeloid Leukemia
Adel A. Hagag1 and Amal Ezzat Abd El-Lateef2
Pediatrics1 and Clinical Pathology2 Departments, Faculty of Medicine, Tanta University, Egypt
Corresponding author: Dr. Adel A Hagag. Pediatrics Department, Faculty of Medicine, Tanta University, Egypt, E-mail:
adelhagag20@yahoo.com
Published: April 20, 2015,
Received: March 4, 2015
Accepted: April 6, 2015
Mediterr J Hematol Infect Dis 2015, 7(1): e2015033, DOI
10.4084/MJHID.2015.033
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/2.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Background: Acute myeloid
leukemia (AML) accounts for 25%-35% of acute leukemia in children.
BAALC gene (Brain and Acute Leukemia Cytoplasmic gene) is a recently
identified gene on chromosome 8q22.3 that has prognostic significance
in AML. The aim of this work was to study the impact of BAALC gene
expression on prognosis of AML in Egyptian children.
Patients and methods: This
study was conducted on 40 Egyptian children with newly diagnosed AML
who were subjected to full history taking, clinical examination and
laboratory investigations including: complete blood count, LDH, bone
marrow aspiration, cytochemistry, immunophenotyping and assessment of
BAALC Gene by real time PCR in bone marrow aspirate mononuclear cells
before the start of chemotherapy.
Results: Positive BAALC
gene expression was found in 24 cases (60%) and negative expression in
16 cases (40%). Positive BAALC gene expression group includes 14 males
and 10 females with mean age at presentation of 8.35±2.63 while
negative BAALC gene expression includes 10 males and 6 females with
mean age at presentation of 7.74±3.23 with no statistically significant
differences between patients with positive and negative BAALC gene
expression regarding age, sex and clinical presentations at time of
diagnosis including pallor, purpura, splenomegaly, hepatomegaly and
lymphadenopathy and laboratory investigations including WBCs and
platelets counts, hemoglobin and LDH levels, and peripheral blood and
bone marrow blast cell counts. There was significant association
between positive BAALC gene expression and M1 and M2 compared with
negative BAALC gene expression which is significantly associated with
M4. There were statistically significant differences in disease outcome
between positive and negative BAALC gene expression groups with higher
rate of relapse and death and lower rate of complete remission and
disease free survival in positive BAALC gene expression group compared
with negative BAALC gene expression group. (p = 0.017).
Conclusion and Recommendation: BAALC
expression is an important bad prognostic factor in AML patients with
normal karyotype and therefore we recommend its incorporation into
novel risk-adapted therapeutic strategies to improve the currently
disappointing cure rate of patients with AML.
|
Introduction
Acute myeloid leukemia (AML) is a clonal malignant disease of the
bone marrow in which hematopoietic progenitor cells are arrested at an
early stage of development due to acquired genetic alterations that
lead to failure of differentiation and to over proliferation.[1] AML
accounts for 25%-35% of the acute leukemia in children.[2]
Over
the past decades, remarkable progress has been made in the treatment
and the understanding of the molecular pathogenesis of acute myeloid
leukemia. At present, up to 65% of pediatric AML patients experience
long-term survival, owing to a more effective use of anti-leukaemic
therapy, improvements in supportive care and better risk
stratification.[1]
It is important to identify prognostic
markers that predict patient's outcome more precisely, thereby allowing
the development of molecular risk-adapted treatment strategies that may
improve the clinical outcome. By the use of molecular genetics
techniques, such as reverse transcriptase polymerase chain reaction
(RT-PCR), global gene expression profiling and/or direct sequencing,
several recurring molecular alterations of prognostic significance have
been identified in patients with cytogenetically normal AML (CN-AML).[3]
BAALC
gene (Brain and Acute Leukemia Cytoplasmic gene), is located on
chromosome 8q22.[3,4] Expression of BAALC was found mainly in
neuroectoderm-derived tissues and hematopoietic precursor cells. In
hematopoietic cells, BAALC expression was restricted to the compartment
of progenitor cells, whereas no expression was detected in mature bone
marrow or circulating white blood cells.[5]
High BAALC gene
expression was found in a subset of patients with AML, acute
lymphoblastic leukemia (ALL), and blast phase of chronic myeloid
leukemia (CML), whereas no BAALC expression could be detected in
patients with chronic-phase CML or chronic lymphocytic leukemia
(CLL).[4] Additionally, high BAALC gene expression occurs in
glioblastoma, melanoma, and childhood gastrointestinal stroma tumors,
suggesting an oncogenic role for BAALC gene. However, the mechanisms
underlying the deregulated expression are unknown.[6]
The
prognostic significance of BAALC gene was first shown in CN-AML with
association with significant higher refractoriness to induction
treatment, lower rates of complete remission (CR), poor overall
survival (OS) and disease free survival (DFS) for patients with high
BAALC expression independent of other prognostic molecular markers with
a gene expression signature consistent with less differentiated AML
blasts.[6-8]
.
Aim of the Work
The aim of this work was to evaluate the prognostic value of BAALC
gene expression in Egyptian children with acute myeloid leukemia.
Subjects and Method
Approval
for this study was granted by the ethical committee of Tanta University
research center and written consent was obtained from the parents of
all children involved in this study. The study participants included 40
Egyptian children with newly diagnosed AML being followed up under the
Oncology Unit of the Pediatric Department in the period from March 2012
to December 2014 including 24 males and 16 females with their ages
ranging from 3-16 years with a mean age value of 9.8±5.8 years. All
patients were subjected to follow up for 2 years to evaluate their
prognosis. Inclusion criteria. Children with cytogenetically normal AML. All patients were subjected to the following:♦ Full history taking. ♦ Thorough clinical examination with special attention to fever, pallor, purpura, hepatomegaly, splenomegaly, and lymphadenopathy.♦ Laboratory investigations Specimen collection and handling.
Three ml venous blood were collected under complete aseptic technique.
They were delivered into 2 tubes: 1 ml blood into a tube containing
EDTA for complete blood count and 2 ml blood into the plain tube for
assessment of Lactate dehydrogenase levels. Two ml of bone marrow
aspirate were drawn into a sterile tube containing EDTA for mononuclear
cell separation for polymerase chain reaction (PCR).Laboratory investigations include the following:♦ Complete blood count.♦ Lactate dehydrogenase (LDH) ♦ Bone marrow aspiration with cytochemical examination and immunophenotyping.♦ Cytogenetic analysisCytogenetic
analyzes of bone marrow or peripheral blood were performed. Metaphase
chromosomes were banded by G-banding technique and Karyotyped according
to the International System for Human Cytogenetic Nomenclature. A
minimum of 20 metaphases was required to be examined for any patient to
be classified as having a normal cytogenetic study.[9] ♦ Assessment of BAALC Gene by real-time PCR. Mononuclear cells were separated from the samples by centrifugation on Density gradient medium.[10]
RNA was isolated using an RNA easy Mini Kit, and the concentration of
extracted RNA was evaluated by spectrophotometry (SPEC).[11]
DNA amplification was done by real-time PCR using Gene Amp 5700
Sequence Detection System. Real-time PCR was used for the detection of
BAALC gene.[12] BAALC
mRNA expression was normalized simultaneously analyzing the
glucose phosphate isomerase (GPI) gene. The relative BAALC expression
was determined using the comparative cycle threshold method. BAALC were
amplified using 1 μL cDNA, 1× master mix (IQ Mix; BioRad, Munich,
Germany).• Glucose phosphate isomerase (GPI) forward primer 5’-TCTTCGATGCCAACAAGGAC-3 • Glucose phosphate isomerase (GPI) reverse primer 5’-GCATCACGTCCTCCGTCAC-3• Glucose phosphate isomerase (GPI) probe -‘HEX-TTCAGCTTGACCCTCAACACCAAC-TAMRA-3’5 • BAALC Gene forward primer:5’-GCCCTCTGACCCAAACAG-3’;• BAALC Gene reverses primer:5’-CTTTTGCAGGCATTCTCTTAGCA-3’;• BALCC Gene probe:5’-FAMCTCTTTTAGCCTCTGTGGT-3’; Reactions were performed using real-time PCR 7000 sequence detection system (Applied Biosystems, Foster City, CA, USA).[12]
A value of 0.166 for BAALC gene was attributed as cut off value, so
BAALC gene expression was considered positive if BAALC gene expression
is above 0.166. On the contrary, BAALC gene expression was considered
negative if BAALC gene expression is below 0.166. Follow up of patients
was carried out clinically and by blast count in BM on day 28 after two
courses of induction therapy according to AML-protocol (MRC10).[13,14]Course 1 (ADE)Aracytin 100 mg/m2 IV bolus every 12 hours on days 1-10 (20 doses), Daunorubicin 50 mg/ m2 IV on days 1, 3, 5 , Etoposide 100 mg/m2 (1 hour IV infusion) on days 1-5 and age adjusted intrathecal Aracytin at time of diagnostic lumber puncture.Course 2 (ADE)Aracytin 100 mg/m2 IV bolus every 12 hours on days 1-8 (16 doses), Daunorubicin 50 mg/m2 IV daily on days 1, 3, 5, Etoposide 100 mg/m2 daily (1 hour IV infusion) on days 1-5 and age-adjusted intrathecal Aracytin on day 1 of course 2.Course 3 (ACE )Aracytin 1gm/m2/dose IV every 12 hours on days 1–5 (10 doses) and Etoposide 150 mg/m2/dose daily (1 hour IV infusion) on days 1–5 with age-adjusted intrathecal Aracytin on day 1 of course 3.Course 4 (MIDAC) Mitoxantrone 10 mg/m2 IV daily (short infusion) days 1-5, Aracytin 1gm/m2/12hours (2 hours IV infusion) on days 1-3 (6 doses) and age-adjusted intrathecal Aracytin on day 1 of course 4.Course 5 (CLASP) Aracytin 3gm/m2 IV every 12 hours on days 1, 2, 8 and 9 (8 doses), L-asparaginase 6,000 IU/m2 IM on days 2 and 9 (3 hours after completion of Aracytin). Age-adjusted
intrathecal chemotherapy with Aracytin: 20 mg for age less than 1 year;
30 mg for age of 1- 2 years; 50 mg for age of 2-3 years and 60 mg for
age of 3 year or older. Statistical Analysis
The
patient’s data were collected and statistically analyzed using
SPSS software statistical computer package version 12. All Data were
expressed as in terms of mean values ± SD. The difference between two
means was statistically analyzed using the student (t) test. A
chi-square test (X2) and Fischer
exact test was used as a test of significance. The log-rank test was
used to assess survival. Significance was adopted at p < 0.05.
Results
Positive BAALC gene expression was found in 24 cases (60%) and negative expression in 16 cases (40%).
Positive
BAALC gene expression group (n=24) includes 14 males and ten females
with a mean age at presentation of 8.35±2.63. Pallor was found in 20
cases, purpura in 22 cases, splenomegaly in 19 cases, hepatomegaly in
16 cases and lymphadenopathy in 8 cases. The negative BAALC gene
expression group (n=16) includes ten males and six females with a mean
age at presentation of 7.74±3.23. In this group pallor was found in 13
cases, purpura in 14 cases, splenomegaly in 13 cases, hepatomegaly in
11 cases and lymphadenopathy in 6 cases. There were no statistically
significant differences between patients with positive and negative
BAALC gene expression regarding age, sex and clinical presentations at
the time of diagnosis (Table 1).
|
|
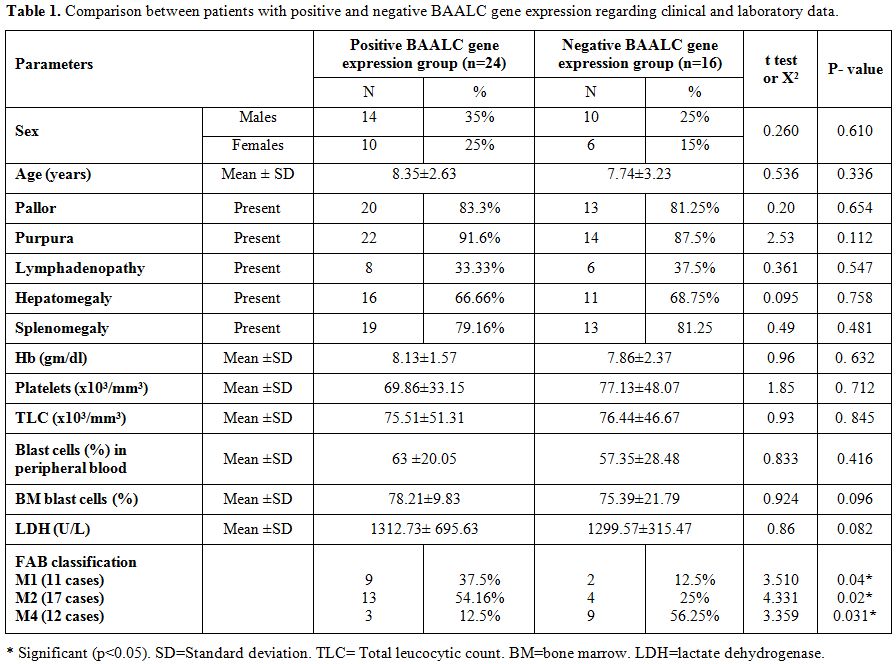
Table 1. Comparison between patients with positive and
negative BAALC gene expression regarding clinical and laboratory
data. |
There were no significant
differences between positive and negative BAALC gene expression groups
regarding WBCs and platelets counts, hemoglobin, and LDH levels, and
peripheral blood and bone marrow blast cell counts. (The mean WBCs
count was 75.51±51.31 in the positive BAALC gene group versus and
76.44±46.67 in the negative BAALC gene group, with a p-value of 0.845.
The mean platelets count was 69.86±33.15 in the positive BAALC gene
expression group versus 77.13±48.07 in the negative BAALC gene group,
with a p-value of 0.712. The mean hemoglobin level was 8.13±1.57 in the
positive BAALC gene group versus 7.86±2.37 in the negative BAALC gene
group, with a p-value of 0.632. The mean LDH level was 1312.73± 695.63
in the positive BAALC gene group versus 1299.57±315.47 in the
negative BAALC gene expression group, with a p-value of 0.082. The mean
peripheral blood blast cells in the positive BAALC gene expression
group was 63 ±20.05 versus 57.35±28.48 in the negative BAALC gene
expression group, with a p-value of 0.416. The mean bone marrow blast
cells in the positive BAALC gene expression group was 78.21±9.83 versus
75.39±21.79 in the negative BAALC gene expression group with p-value of
0.096) (Table 1).
There was a significant association
between positive BAALC gene expression and M1 and M2 subtypes compared
with negative BAALC gene expression significantly associated with the
M4 subtype. In fact, of 24 cases with positive BAALC gene expression; 9
were M1, 13 were M2, and 3 M4 whereas of 16 patients with negative
BAALC gene expression; 2 were M1, 4 M2, and 9 M4. The presence of
positive and negative BAALC was statistically different in the FAB
subtypes) (Table 1).
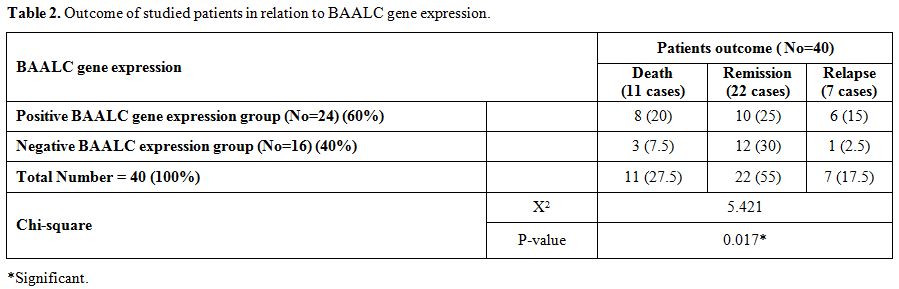
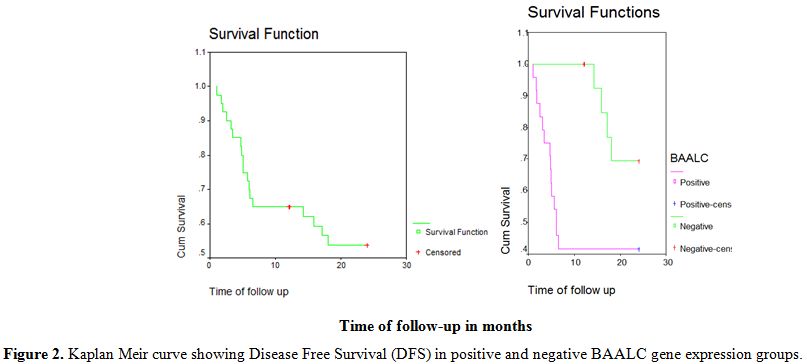
There was a statistically significant
difference in disease outcome between positive and negative BAALC gene
expression groups with higher rate of relapse and death and lower rate
of complete remission and disease free survival in positive BAALC gene
expression group compared with negative BAALC gene expression group. (p
= 0.017). Of 24 patients positive; 10 achieved complete remission, 8
died and 6 suffered from relapse, while of 16 patients negative; 12
achieved complete remission, 1 suffered from relapse and 3 died with a
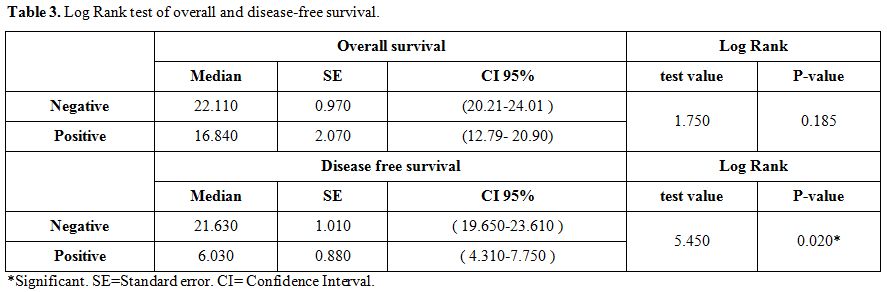
median disease-free survival in the positive group of 6.03 months
compared with 21.63 months in negative group (Table 2, 3 and Figure 1, 2).
|
|
Table 2. Outcome of studied patients in relation to BAALC gene expression. |
|
|
Table 3. Log Rank test of overall and disease-free survival. |
|
|
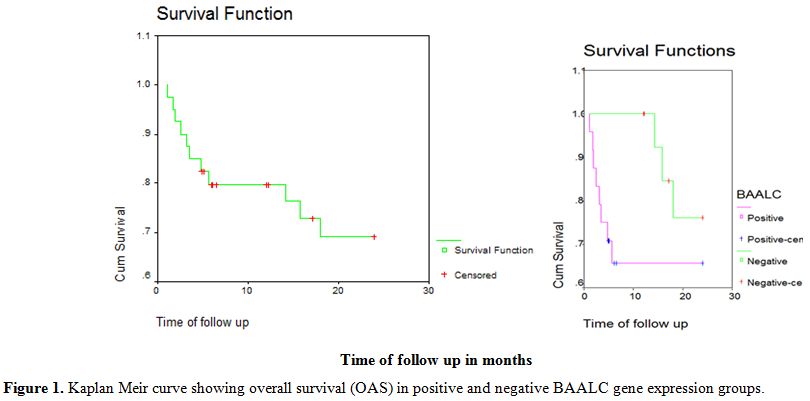
Figure 1. Kaplan Meir curve showing overall survival (OAS) in positive and negative BAALC gene expression groups. |
|
|
Figure 2. Kaplan Meir curve showing Disease Free Survival (DFS) in positive and negative BAALC gene expression groups. |
Discussion
Acute myeloid leukemia is a
clonal malignant disease of hematopoietic tissue that is characterized
by the proliferation of abnormal myeloblast cells principally in marrow
and impaired production of normal blood cells.[15]
The prognosis of AML varies dramatically and is strongly influenced by
a number of factors, including age, performance status, and cytogenetic
and/or molecular alterations.[16]
In recent
years, a major focus of molecular cancer research has been the analysis
of genes that may be the cause of carcinogenesis (oncogenes).[17] Multiple chromosomal and gene rearrangements have been identified in AML, such as MLL, PML/RARA, DEK/CAN, and AML1/ETO.[18]
Chromosomal rearrangements involving the MLL gene at band 11q23 are the
most common genetic alteration encountered in infant acute myeloid
leukemia. Reciprocal translocation represents the most frequent form of
MLL rearrangement.[19] NRAS mutation varies
considerably in patients with childhood AML and was found in about 15%
of pediatric AML patients in some studies.[17,20]
The
present study was designed to use Real-time PCR analysis to study the
prognostic value of BAALC gene expression in Egyptian children with
AML.
In this study, positive BAALC gene expression was found in 24 cases (60%).This is in substantial accord with Yahya et al 2013,[21] who found high BAALC gene expression in 22 of 45 patients (48.9%) and Damiani et al 2013,[22] who found BAALC gene overexpression in 87/175 (50%) of their studied patients.
In
the present study, there were no statistically significant differences
between patients with positive and negative BAALC gene expression
regarding age, sex and clinical presentation at time of diagnosis
including pallor, purpura, hepatomegaly, splenomegaly, and
lymphadenopathy. These results were in agreement with Yahya et al. 2013[21]
who found no significant differences between positive and negative
BAALC gene expression regarding clinical parameters of patients at the
time of diagnosis.
In this work, there were no significant
differences between positive and negative BAALC gene expression
regarding WBCs and platelets counts, hemoglobin, and LDH levels, and
blast cell counts in the peripheral blood and bone marrow. This is in
agreement with Elsharnouby et al. 2010[23] who found
no significant differences between positive and negative BAALC gene
expression regarding WBCs and platelets counts, hemoglobin, and LDH
levels, blast cell counts, both in the peripheral blood and bone
marrow. But not in agreement with Baldus et al. 2003[24]
who found the association between positive BAALC gene expression and
significantly higher WBCs and blast cell counts in the peripheral blood
and bone marrow.
Variation between the results of this study and
the previous studies may be explained by different age and number of
studied patients, different localities, different presentations of
leukemia, different duration of studies and different duration of
follow-up.
In the current study, there was a significant
association between BAALC gene expression and certain FAB subtypes with
predominant positive BAALC gene expression in M1 and M2 and predominant
negative BAALC gene expression in M4. These data are in agreement with
Bienz et al 2005[26] and Elsharnouby et al 2010[23] who both found high BAALC expression more frequently in M1, M2 and less in M4, M5, and Yanaihara et al 2006[25] who stated that high BAALC gene expression is more often present in M1.
In
our study there were statistically significant differences in disease
outcome between positive and negative BAALC gene expression groups with
higher rate of relapse and death and lower rate of complete remission
and disease free survival in positive BAALC gene expression group
compared with negative BAALC gene expression group. This is in
agreement with Nibourel et al 2010[27] who stated that BAALC gene expression was found to be an independent negative prognostic factor in CN-AML, Yahya et al 2013[21]
who found that high BAALC expression had significantly lower incidence
of CR, higher mortality rate, significantly shorter DFS, and inferior
overall survival, Weber et al 2014[28] who revealed
an independent adverse prognostic impact of high BAALC expression on
overall survival and event-free survival and Damiani et al 2013[22]
who found that overexpression of BAALC gene confers poor prognosis in
cytogenetically normal AML patients, with negative impact on CR
achievement, overall survival but have no influence on relapse
probability.
Conclusion and Recommendation
BAALC expression is an important bad prognostic factor in AML
patients with normal karyotype, and therefore we recommend its
incorporation into novel risk-adapted therapeutic strategies to improve
the currently disappointing cure rate of patients with AML.
References
- Arber DA, Brunning RD, Orazi A, Le Beau M.
Acute myeloid leukemia with myelodysplasia-related changes. In:
Swerdlow SH, Campo E, Harris NL (eds.), WHO Classification of Tumors of
Hematopoietic and Lymphoid Tissues. (4thedition). 2008b: 124-126.
- Juliusson
G, Lazarevic VL, Horstedt AS, Hagberg O, Höglund M, Swedish Acute
Leukemia Registry Group. Acute myeloid leukemia in the real word: Why
population- based registries are needed. Blood 2012 Apr 26;
119(17):3890-9. doi: 10.1182/blood-2011-12-379008. Epub 2012 Mar 1. http://dx.doi.org/10.1182/blood-2011-12-379008
 .
. - Mro
zek K, Marcucci G, Paschka P, Whitman SP, Bloomfield CD. Clinical
relevance of mutations and gene-expression changes in adult acute
myeloid leukemia with normal cytogenetics: Are we ready for a
prognostically prioritized molecular classification? Blood 2007;
109:431-448. http://dx.doi.org/10.1182/blood-2006-06-001149 PMid:16960150 PMCid:PMC1785102 .
- Tanner
SM, Austin JL, Leone G, Rush LJ, Plass C, Heinonen K, Mrózek K, Sill H,
Knuutila S, Kolitz JE, Archer KJ, Caligiuri MA, Bloomfield CD, de La
Chapelle. BAALC, the human member of a novel mammalian neuroectoderm
gene lineage, is implicated in hematopoiesis and acute leukemia. Proc
Natl Acad Sci USA 2001 Nov 20; 98(24):13901-6. Epub 2001 Nov 13. http://dx.doi.org/10.1073/pnas.241525498 PMid:11707601 PMCid:PMC61139 .
- Ilencíková
D, Sykora J, Mikulaon Z Repiská V. Identification of molecular markers
in children with acute myeloid leukemia. Clin Oncol. 2012; 25(1):26-35. .
- Eisfeld
AK, Marcucci G, Liyanarachchi S, Döhner K, Schwind S, Maharry K, Leffel
B, Döhner H, Radmacher MD, Bloomfield CD, Tanner SM, de la Chapelle A.
. Heritable polymorphism predisposes to high BAALC expression in acute
myeloid leukemia. Proc Natl Acad Sci USA 2012 Apr 24; 109(17):6668-73.
Epub 2012 Apr 9. http://dx.doi.org/10.1073/pnas.1203756109 .
- Baldus
CD, Martus P, Burmeister T, Schwartz S, Gökbuget N, Bloomfield CD,
Hoelzer D, Thiel E, Hofmann WK. Low ERG and BAALC expression identifies
a new subgroup of adult acute T Lymphoblastic leukemia with a highly
favorable outcome. J Clin Oncal. 2007 Aug 20; 25(24):3739-45. Epub 2007
Jul 23. http://dx.doi.org/10.1200/JCO.2007.11.5253 PMid:17646667 .
- Santamaría
C, Chillón MC, García-Sanz R, Pérez C, Caballero MD, Mateos MV, Ramos
F, de Coca AG, Alonso JM, Giraldo P, Bernal T, Queizán JA, Rodríguez
JN, Puig N, Balanzategui A, Sarasquete ME, Alcoceba M, Díaz-Mediavilla
J, San Miguel J, González M. BAALC is an important predictor of
refractoriness to chemotherapy and poor survival in intermediate-risk
acute myeloid leukemia. Ann Hematol. 2010 May; 89(5):453-8. Epub 2009
Nov 27. http://dx.doi.org/10.1007/s00277-009-0864-x .
- Byrd
JC, Mrózek K, Dodge RK, Carroll AJ, Edwards CG, Arthur DC, Pettenati
MJ, Patil SR, Rao KW, Watson MS, Koduru PR, Moore JO, Stone RM, Mayer
RJ, Feldman EJ, Davey FR, Schiffer CA, Larson RA, Bloomfield CD; Cancer
and Leukemia Group B (CALGB 8461). Pretreatment cytogenetic
abnormalities are predictive of induction success, cumulative incidence
of relapse, and overall survival in adult patients with de novo acute
myeloid leukemia: Results from Cancer and Leukemia Group B (CALGB
8461). Blood 2002 Dec 15; 100(13):4325-36. Epub 2002 Aug 1. http://dx.doi.org/10.1182/blood-2002-03-0772 PMid:12393746 .
- Boyam
A. Isolation of mononuclear cells and granulocytes from human blood.
Isolation of monuclear cells by one centrifugation and of granulocytes
by combining centrifugation and sedimentation at 1g. Scand J Clin Lab
Invest Suppl. 1968; 97:77-89 .
- Guo
X, Shi P, Chen F, Zha J, Liu B, Li R, Dong H, Zheng H, Xu B. Low MDR1
and BAALC expression identifies a new subgroup of intermediate
cytogenetic risk acute myeloid leukemia with a favorable outcome. Blood
Cells Mol Dis. 2014 Sep; 53(3):144-8. Epub 2014 May 20. http://dx.doi.org/10.1016/j.bcmd.2014.05.001 .
- Baladus
A., Thiede C, Soucek S. BAALC expression and FLT-3 internal tandem
duplication mutations in acute myeloid leukemia patients with normal
cytogenetic: Prognostic implications .J Clin Oncol. 2006; 24:790-7. http://dx.doi.org/10.1200/JCO.2005.01.6253 PMid:16418499 .
- Hann
IM, Webb DK, Gibson BE, Harrison CJ. MRC trials in childhood acute
myeloid leukaemia. Ann Hematol. 2004; 83 (Suppl 1):
S108-12. PMid:15124698 .
- Gibson
BE, Webb DK, Howman AJ, De Graaf SS, Harrison CJ, Wheatley K; United
Kingdom Childhood Leukaemia Working Group and the Dutch Childhood
Oncology Group. Results of a randomized trial in children with Acute
Myeloid Leukemia: medical research council AML12 trial. Br J Haematol.
2011 Nov; 155(3):366-76. Epub 2011 Sep 9. http://dx.doi.org/10.1111/j.1365-2141.2011.08851.x .
- Ishikawa
Y, Kiyoi H, Naoe T. Prevalence and clinical characteristics of
N-terminally truncated WT1 expression in acute myeloid leukemia. Leuk
Res. 2011 May; 35(5):685-8. Epub 2011 Jan 21. http://dx.doi.org/10.1016/j.leukres.2011.01.002 .
- Döhner
H, Estey EH, Amadori S, Appelbaum FR, Büchner T, Burnett AK, Dombret H,
Fenaux P, Grimwade D, Larson RA, Lo-Coco F, Naoe T, Niederwieser D,
Ossenkoppele GJ, Sanz MA, Sierra J, Tallman MS, Löwenberg B, Bloomfield
CD, European Leukemia Net. Diagnosis and management of AML in adults:
Recommendation from an international expert panel, on behalf of the
European leukemia net. Blood 2010 Jan 21; 115(3):453-474. Epub
2009 Oct 30. http://dx.doi.org/10.1182/blood-2009-07-235358 .
- Aly
RM, El-Sharnoby MR, Hagag AA. Prognostic Significance of NRAS Gene
Mutations in Children with Acute Myelogenous leukemia. Mediterr J
Hematol Infect Dis. 2011; 3(1):e2011055. http://dx.doi.org/10.4084/mjhid.2011.055 .
- Mrózek
K, Heinonen K, Bloomfield CD. Clinical importance of cytogenetics in
acute myeloid leukemia. Best Pract Res Clin Haematol. 2001; 14:19-47. http://dx.doi.org/10.1053/beha.2000.0114 PMid:11355922 .
- Launay
E, Henry C, Meyer C, Chappé C, Taque S, Boulland ML, Ben Abdelali R,
Dugay F, Marschalek R, Bastard C, Fest T, Gandemer V, Belaud-Rotureau
MA. MLL-SEPT5 fusion transcript in infant acute myeloid leukemia with
t(11;22)(q23;q11). Leuk Lymphoma 2014 Mar; 55(3):662-7. http://dx.doi.org/10.3109/10428194.2013.809528 .
- Liang
DC, Shih LY, Fu JF, Li HY, Wang HI, Hung IJ, Yang CP, Jaing TH, Chen
SH, Liu HC. K-ras mutations and N-ras mutations in childhood acute
leukemias with or without mixed-lineage leukemia gene rearrangements.
Cancer 2006; 106: 950-956. http://dx.doi.org/10.1002/cncr.21687 PMid:16404744. .
- Yahya
RS, Sofan MA, Abdelmasseih HM, Saudy N, Sharaf-Eldein MA. Prognostic
implication of BAALC gene expression in adult acute myeloid leukemia
Clin Lab. 2013; 59(5-6):621-8. PMid:23865362 .
- Damiani
D, Tiribelli M, Franzoni A, Michelutti A, Fabbro D, Cavallin M,
Toffoletti E, Simeone E, Fanin R, Damante G. BAALC overexpression
retains its negative prognostic role across all cytogenetic risk groups
in acute myeloid leukemia patients. Am J Hematol. 2013 Oct;
88(10):848-52. Epub 2013 Jul 23. http://dx.doi.org/10.1002/ajh.23516 .
- El-Sharnouby
JA, Sayed Ahmed LM, Taha AM, Okasha K. Prognostic Significance of CEBPA
Mutations and BAALC Expression in Acute Myeloid Leukemia Patients with
Normal Karyotype. Eur J Gen Med. 2010; 7(1):17-28. .
- Baldus
CD, Tanner SM, Ruppert AS, Whitman SP, Archer KJ, Marcucci G, Caligiuri
MA, Carroll AJ, Vardiman JW, Powell BL, Allen SL, Moore JO, Larson RA,
Kolitz JE, de la Chapelle A, Bloomfield CD. BAALC expression predicts
clinical outcome of de novo acute myeloid leukemia patients with normal
cytogenetic: A Cancer and Leukemia Group B study. Blood 2003 Sep 1;
102(5):1613-8. Epub 2003 May 15. http://dx.doi.org/10.1182/blood-2003-02-0359 PMid:12750167 .
- Yanaihara
N, Caplen N, Bowman E, Seike M, Kumamoto K, Yi M, Stephens RM, Okamoto
A, Yokota J, Tanaka T, Calin GA, Liu CG, Croce CM, Harris CC. Unique
microRNA molecular profiles in lung cancer diagnosis and prognosis.
Cancer Cell 2006 Mar; 9(3):189-98. http://dx.doi.org/10.1016/j.ccr.2006.01.025 PMid:16530703 .
- Bienz
M, Ludwig M, Leibundgut EO, Mueller BU, Ratschiller D, Solenthaler M,
Fey MF, Pabst T. Risk assessment in patients with acute myeloid
leukemia and a normal karyotype. Clin Cancer Res. 2005 Feb 15;
11(4):1416-24. http://dx.doi.org/10.1158/1078-0432.CCR-04-1552 PMid:15746041 .
- Nibourel
O, Kosmider O, Cheok M, Boissel N, Renneville A, Philippe N, Dombret H,
Dreyfus F, Quesnel B, Geffroy S, Quentin S, Roche-Lestienne C, Cayuela
JM, Roumier C, Fenaux P, Vainchenker W, Bernard OA, Soulier J, Fontenay
M, Preudhomme C. Incidence and prognostic value of TET2 alterations in
de novo acute myeloid leukemia achieving complete remission. Blood 2010
Aug 19; 116(7):1132-5. Epub 2010 May 20. http://dx.doi.org/10.1182/blood-2009-07-234484 .
- S
Weber, T Alpermann, F Dicker, S Jeromin, N Nadarajah, C Eder, A Fasan1,
A Kohlmann, M Meggendorfer, C Haferlach, W Kern, T Haferlach and S
Schnittger. BAALC expression: a suitable marker for prognostic risk
stratification and detection of residual disease in cytogenetically
normal acute myeloid leukemia. Blood Cancer Journal 2014 January 10; 4,
e173; doi:10.1038/bcj.2013.71. http://dx.doi.org/10.1038/bcj.2013.71 .
[TOP]