Received: August 23, 2015
Accepted: November 11, 2015
Mediterr J Hematol Infect Dis 2016, 8(1): e2016010, DOI 10.4084/MJHID.2016.010
This article is available on PDF format at:

Alexei Shimanovsky1, Devbala Patel2 and Jeffrey Wasser1
| This is an Open Access article distributed
under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
|
Abstract Immune thrombocytopenic purpura (ITP)
is characterized by a decreased platelet count caused by excess
destruction of platelets and inadequate platelet production. In many
cases, the etiology is not known, but the viral illness is thought to
play a role in the development of some cases of ITP. The current (2011)
American Society of Hematology ITP guidelines recommend initial
diagnostic studies to include testing for HIV and Hepatitis C. The
guidelines suggest that initial treatment consist of observation,
therapy with corticosteroids, IVIG or anti D. Most cases respond
to the standard therapy such that the steroids may be tapered and the
platelet counts remain at a hemostatically safe level. Some patients
with ITP are dependent on long-term steroid maintenance, and the
thrombocytopenia persists with the tapering of the steroids. Recent
case reports demonstrate that ITP related to cytomegalovirus (CMV) can
persist in spite of standard therapy and that antiviral therapy may be
indicated. Herein we report a case of a 26-year-old female with
persistent ITP that resolved after the delivery of a CMV-infected
infant and placenta. Furthermore, we review the current literature on
CMV-associated ITP and propose that the current ITP guidelines be
amended to include assessment for CMV, even in the absence of signs and
symptoms, as part of the work-up for severe and refractory ITP,
especially prior to undergoing an invasive procedure such as
splenectomy. |
Introduction
Immune thrombocytopenic purpura (ITP) is a common cause of acquired
thrombocytopenia caused by auto-anti-platelet antibodies that destroy
platelets, damage megakaryocytes and inhibit platelets
production. Viral infection such as rubella, varicella, mumps,
cytomegalovirus (CMV) and Epstein-Barr virus are linked to ITP and
thrombocytopenia.[1] While the infections can be
relatively asymptomatic, they can trigger an autoimmune process. In the
past several years, cases of ITP have been reported secondary to
unsuspected, persistent infections such as hepatitis C, HIV and Helicobacter pylori (H. pylori). The successful treatment of ITP in such cases may require recognition and eradication of the underlying infection.
Several
cases of thrombocytopenia and ITP, secondary to persistent CMV
infection, in immunocompetent adults, have been reported in the
literature.[2] While the majority of cases describe
patients that responded to standard ITP therapy, some reports describe
patients who are dependent upon or worsen with corticosteroids.[2-5]
In a small case-series of four patients, steroids appeared to worsen
CMV-associated ITP and improvement in the platelet counts occurred
after starting gancyclovir and Cytogam with steroid taper.[6]
Herein we describe a case of an immunocompetent adult female diagnosed
with ITP, refractory to standard therapy, during her first pregnancy.
The ITP improved following delivery of a CMV-infected neonate and the
products of conception. The placenta demonstrated evidence of
active CMV infection by PCR. Furthermore, we review current
literature and propose a modification to the current ITP guidelines.
Case Report
A healthy 26-year-old G1P0 female of Asian-Indian descent was
referred to our clinic for a second opinion of her thrombocytopenia.
During her initial visit to the obstetrician, she was asymptomatic and
had a platelet count of 3 x 109/l (normal 150-450 x 109/l).
She initially received intravenous immunoglobulin (IVIG) at 1 g/kg,
prednisone 140 mg/day and a trial of anti-D. Her platelet count
improved temporarily, returning to 10-30x109//l after a few weeks (Figure 1). She was on maintenance prednisone (40 mg/day) when she first presented to our clinic.
The
patient denied having an abnormal menstrual cycle, mucosal bleeding,
and family history of blood disorders. On physical exam, the patient
appeared cushingoid with normal vital signs. She had no petechiae or
ecchymosis. Uterus was gravid. She had no palpable hepatosplenomegaly.
The rest of her exam was normal. The leucocyte count was
24,500/uL, with 7% band forms, 88% neutrophils, and 4% lymphocytes. The
hemoglobin was 13 g/dL with a hematocrit of 37%. Her platelet count was
30x109/l. Coagulation screen, liver
profile, and blood chemistry values were normal. Bone marrow biopsy
showed megakaryocyte hyperplasia with normal morphology, consistent
with ITP. Her ANA, Hepatitis B, C, and HIV were negative. Stool H. pylori antigen was positive.
The
patient was treated with pantoprazole 40 mg daily, amoxicillin 1000 mg
daily and clarithromycin 500 mg twice daily. After treatment, her
platelet count remained between 10-40x109//l. As resistance to H. pylori treatment is common, the patient received a second course of antibiotic therapy. Subsequently, the H. pylori
stool antigen became negative with no improvement in platelet count.
After receiving appropriate vaccinations, she underwent a splenectomy
with no improvement in platelet count. She was maintained on prednisone
40 mg/day and intermittent IVIG until her delivery.
She delivered a healthy baby girl with a platelet count of 15x109//l
and no significant hemorrhage or bleeding. During a routine screen, the
infant was diagnosed with congenital CMV via urine PCR. The newborn was
treated with ganciclovir 10mg/kg, leading to improvement in platelet
count. Placental pathology demonstrated focal chorionic chorionitis
without any chorionic villinits. The corresponding segment of the
placenta was positive for CMV by PCR. The mother was positive for CMV
IgG. Interestingly, one week after delivery, the patient’s platelet
count began to improve. She was no longer taking prednisone or IVIG and
her platelet count normalized to 192x109/l ten months after delivery (Figure 1).
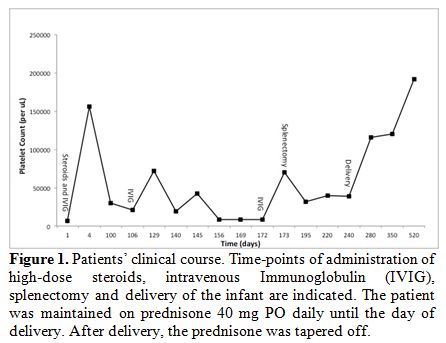 |
Figure 1. Patients’ clinical course. Time-points of administration of high-dose steroids, intravenous Immunoglobulin (IVIG), splenectomy and delivery of the infant are indicated. The patient was maintained on prednisone 40 mg PO daily until the day of delivery. After delivery, the prednisone was tapered off. |
Discussion
Our patient presented with severe thrombocytopenia in her first
trimester of pregnancy. While gestational thrombocytopenia accounts for
70-80% of cases during pregnancy, our patient did not meet the clinical
criteria for this diagnosis. Her platelet count was less than 100x109/l and she presented early in pregnancy, findings that are less consistent with gestational thrombocytopenia.[7]
While type 2B von Willebrand was considered in the differential of
thrombocytopenia in our patient, it is less likely in our patient as
she did not have any personal or family history of abnormal bleeding.
Given the normal vital signs and liver function, pregnancy-specific
causes of thrombocytopenia such as preeclampsia, eclampsia, HELLP
syndrome and acute fatty liver are less likely. Moreover, the patient’s
bone marrow was consistent with ITP and the temporary response to
corticosteroids and IVIG supports the diagnosis of ITP.
ITP is a
rare cause of thrombocytopenia during pregnancy, occurring only 1 in
10,000 pregnancies. While ITP can occur at any point in pregnancy, it
is one of the few causes of thrombocytopenia that can become apparent
during the first trimester.[8] Primary ITP is
caused by a complex mechanism that is caused by autoantibodies against
platelets and T-cell mediated platelet destruction.[9] Conversely, secondary ITP develops in a setting of autoimmune disease, lymphoma, and infection with H. pylori or viral infection such as HIV, hepatitis C, or CMV.[7]
The
current ITP guidelines from the American Society of Hematology
recommend testing for Hepatitis C and HIV, as they are known to cause
secondary ITP.[10] Both were negative in our patient. Testing for H. pylori is also recommended in patients with isolated thrombocytopenia. The stool antigen for H. pylori positive in our patient and we considered H. pylori-associated
ITP however; the patients’ platelets did not improve after two courses
of triple antibiotic therapy. The patient was treated based on the
current guidelines with corticosteroids, IVIG, and splenectomy. Except
a temporary spike in her platelet count (Figure 1) after IVIG administration, the patient failed to have a durable response to standard therapy.
After
delivery, the patient’s newborn was diagnosed with congenital CMV.
While CMV is known to cause secondary ITP, isolated thrombocytopenia,
and fetal damage, in most countries pregnant women are not routinely
screened for CMV.[11] Indeed, neither the American
Society of Obstetrics and Gynecology (ACOG) nor the Centers for Disease
Control and Prevention (CDC) recommend routine serologic screening for
CMV in pregnant women.[12] Furthermore, the current ITP guidelines from the American Society of Hematology do not require CMV testing.[10]
Consequently, medical insurance companies may refuse to cover the costs
of CMV testing in patients that have isolated thrombocytopenia and do
not exhibit symptoms that suggest CMV. Indeed, in the United States,
isolated thrombocytopenia is not considered to be reimbursable
indication for CMV testing by Medicare and insurers may refuse payment
for asymptomatic patients.
While some experts recommend testing
for CMV in thrombocytopenic patients that have lymphocytosis, atypical
lymphocytes, toxic granulation or neutrophilia, our patient had none of
these signs of CMV infection.[7] As such, our patient
was not tested for CMV during her pregnancy and the diagnosis of
CMV-associated ITP was only considered in our patient postpartum, when
the fetal urine and placenta tested positive for CMV infection.
The
patient’s clinical course and bone marrow findings suggest that the
persistent thrombocytopenia was due to secondary ITP caused by CMV
infection. We propose that the mother either acquired CMV infection
early in pregnancy or had a reactivation of the virus leading to
symptomatic CMV causing her to have thrombocytopenia and ITP. Moreover,
we hypothesize that the placenta was a reservoir for CMV, thus causing
persistent ITP that was refractory to standard therapy, resolving only
after delivery. Indeed, mammalian models have demonstrated that the
placenta can act as a reservoir for CMV long after it is cleared from
the maternal blood.[13] Soon after the delivery, the CMV reservoir was removed, and maternal platelet count returned to normal levels.
Cytomegalovirus infection in an immunocompetent host is frequently asymptomatic and detected retrospectively.[14]
Increasing evidence from the recent literature suggests that CMV
infection may be associated with ITP, especially refractory ITP.[2] A study by Sheng Yu et al. showed that CMV infection, especially the gB1 genotype, was the cause of ITP in children.[15]
A recent review by DiMaggio et al., suggests that CMV may be the cause
of severe and refractory ITP and that CMV PCR should be ordered if
there is a strong clinical suspicion of an infection.[6,16] To date, 9 cases of severe, steroid-resistant CMV-associated thrombocytopenia and ITP have been reported (Table 1) in immunocompetent adults.[2-6,17-20] In some of the cases, thrombocytopenia associated with CMV-induced ITP worsened after administration of steroid therapy.[6,15]
Although
the mechanism of CMV-induced thrombocytopenia is unclear, several
hypotheses have been proposed. Molecular mimicry leading to the
production of anti-platelet antibodies causing immune dysregulation and
platelet destruction is one such mechanism.[21]
Additionally, CMV directly infects megakaryocytes leading maturation
arrest causing decreased platelet production and thrombocytopenia.[21] Indeed, this has been described as the cause of delayed platelet recovery following allogeneic bone marrow transplant.[22]
Furthermore, the latter better explains the lack of a durable response
with corticosteroids, as this therapy is aimed at blocking platelet
destruction and not increasing platelet production.[23]
Accordingly, in non-pregnant patients, a trial of a thrombomimetic
agent may be useful in severe refractory cases of ITP. Moreover,
treatment with ganciclovir and Cytogam to optimize rapid suppression of
CMV may provide greater efficacy and faster clinical improvement.
Indeed, treatment with anti-CMV therapy has produced a rise in platelet
count and improvement in clinical outcome in some patients with
CMV-associated ITP.[5,6,19,20]
The current case and literature reports (Table 1)
suggest that CMV-associated ITP can cause severe thrombocytopenia
refractory to standard therapy and treatment of the underlying CMV
infection may improve thrombocytopenia. However, while some clinicians
check for CMV in patients with thrombocytopenia, the current American
Society of Hematology (2011) guidelines for the diagnosis and
management of ITP recommend checking and treating only for Hepatitis C
and HIV; they do not recommend testing for CMV as part of the
diagnostic workup, representing a gap in the current guidelines.[10]
We believe it is appropriate to test for CMV infection if there is a
high clinical suspicion of CMV exposure, steroid-dependent ITP or
before splenectomy. Moreover, treatment with ganciclovir and Cytogam
should be further investigated in non-pregnant individuals where
CMV-associated ITP is suspected. Accordingly, modification of the
American Society of Hematology ITP guidelines and those of other
organizations may be warranted. Those modifications should include
recommendations for CMV testing in pregnancy and prior to splenectomy
since treatment of CMV may improve ITP and eliminate the need for
invasive surgery. In addition, this would lead to increase physician
awareness of CMV-induced ITP and may encourage reimbursement for CMV
testing in patients with isolated ITP, who lack other signs and
symptoms of CMV infection. Lastly, clinical trials are needed to
investigate the risk-benefit of treating CMV-induced ITP with
anti-viral agents in pregnant and non-pregnant individuals.
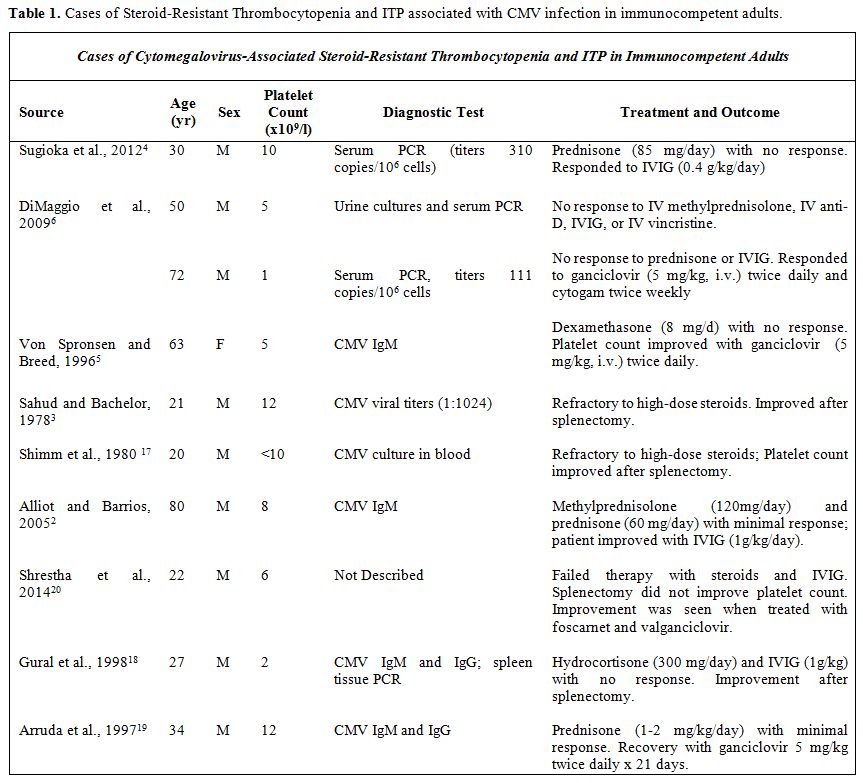 |
Table 1. Cases of Steroid-Resistant Thrombocytopenia and ITP associated with CMV infection in immunocompetent adults. |
References

[TOP]