Elmoubasher Farag1*, Devendra Bansal2, Mohamad Abdul Halim Chehab3, Ayman Al-Dahshan3, Mohamed Bala3, Nandakumar Ganesan1, Yosuf Abdulla Al Abdulla4, Mohammed Al Thani1, Ali A. Sultan2 and Hamad Al-Romaihi1.
1 Ministry of Public Health, Doha, Qatar.
2 Department Microbiology and Immunology, Weill Cornell Medical College in Qatar, Cornell University, Doha, Qatar.
3 Community medicine residency program, Hamad Medical Corporation, Doha, Qatar.
4 Consultant physician, Primary Health Care Corporation, Doha, Qatar.
Correspondence to: Elmoubasher Farag. Ministry of Public Health, Doha, Qatar. E-mail:
eabdfarag@moph.gov.qa
Published: September 1, 2018
Received: May 4, 2018
Accepted: August 3, 2018
Mediterr J Hematol Infect Dis 2018, 10(1): e2018050 DOI
10.4084/MJHID.2018.050
This article is available on PDF format at:

This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
|
Abstract
Background
and Objectives. Imported malaria poses a serious public health problem
in Qatar because its population is “naïve” to such infection; where
local transmission might lead to serious, life-threatening infection
and might even trigger epidemics.
Methods. This study is a
retrospective review of the imported malaria cases in Qatar reported by
the malaria surveillance program at the Ministry of Public Health
(MoPH), during the period between January 2008 and December 2015. All
cases were imported and underwent parasitological confirmation through
microscopy.
Results. A total of 4092 malaria cases were reported
during 2008-2015 in Qatar. The demographic features of the imported
cases show that the majority of cases were males (93%), non-Qatari
(99.6%), and aged 15 to 44 years (82.1%). Moreover, P. vivax was found
to be the main etiologic agent accounting for more than three-quarters
(78.7%) of the imported cases. In addition, almost a third (33.1%) of
the cases were reported during the months of July, August, and
September.
Conclusions. Imported malaria in Qatar has witnessed an
increase during the past seven years, despite a long period of constant
reduction; where the people most affected were adult male migrants from
endemic countries. Many challenges need to be overcome to prevent the
reintroduction of malaria into the country.
|
Introduction
The
global importance of malaria is immense. It is the most prevalent
vector-borne disease in the world, threatening some 2-3 billion people
in more than 90 countries - 56% of the world's population. In 2016, the
World Health Organization estimated that there were 216 million malaria
cases and 445 000 deaths attributable to malaria.[1]
Most of these deaths occurred in the African region (91%), followed by
the South-East Asian region (7%) and the Eastern Mediterranean region
(2%).[2] The vast majority of deaths occurred among
young children; other high-risk groups included pregnant women,
non-immune travelers, refugees, displaced persons, and laborers
entering endemic areas.[3] It is a well-known fact
that both tourists and visiting friends and relatives (VFR) are at high
risk of malaria as they are less likely to use chemoprophylaxis.[4,5]
Moreover, those VFR are at an increased risk of travel-related
diseases, have lower risk perception and awareness, don’t seek
pre-travel advice, and are more likely to reside in remote rural areas
when compared with tourists to the same destinations.[5]
Qatar
is a country (population 2,235,355 in 2015) located in the west of the
Arabian Peninsula. Even though indigenous malaria transmission has been
eliminated in the1970s, the risk of imported malaria still exists due
to the massive influx of migrant workers from the Indian subcontinent
and Sub-Saharan Africa.[6,7] Moreover, this influx has recorded a 9-fold increase between 1995 and 2014.[8]
Additionally, the potential of malaria reintroduction in the country
exists due to the presence of two malaria vectors, namely: A. stephensi and A. multicolor.
The incidence of malaria was found to be in a consistent decline from
1997 to reach the lowest rate in 2004 but then increased by more than
two times in 2005 and 2006.[7] In 2008, approximately 200-250 cases of imported malaria were reported, and P. vivax
was the main etiologic agent. Furthermore, all the patients had a
travel history to malaria-endemic countries as India, Pakistan, and
Sudan.[9] Consequently, imported malaria poses a
serious public health problem in Qatar because the population is
“naïve” to such infection; where local transmission might lead to
serious, life-threatening infection and could even trigger epidemics.
Currently,
information regarding malaria surveillance in Qatar is insufficient to
provide a clear epidemiological picture necessary for the development
of a national strategy to control malaria importation. Therefore, the
country is at risk of such disease and requires robust surveillance and
preparedness to address any potential outbreaks. Thus, in the present
retrospective study, we build a record of data regarding the incidence
of malaria in Qatar to stall the potential spread of this deadly
infection in Qatar.
Materials and Methods
This
study is a retrospective review of the imported malaria cases in Qatar
reported by the malaria surveillance program at the Ministry of Public
Health (MoPH), during the period between January 2008 and December
2015. Hamad Medical Corporation (HMC) is the main health care facility
catering for the population of Qatar and epidemiologically represents
both locals and expatriates in the country; where the hematological
laboratory at HMC is considered to be the national reference
laboratory. All the malaria cases in the present study were reported
from the highly specialized hospitals of HMC: Hamad General Hospital,
Al-Wakrah Hospital, and Al-Khor Hospital. Other sources of malaria
cases were Qatar’s primary health care provider, Primary Health Care
Corporation (PHCC), through its 23 centers as well as the hospitals and
health centers of the private sector.
Malaria Case Management.
In Qatar, the management of malaria cases is centralized under HMC, the
main and government-based provider of secondary and tertiary care in
the country. Malaria cases are typically seen in the emergency
department and triaged accordingly as uncomplicated or complicated
cases based on specific case definitions. Patients infected with P. falciparum / P. vivax having different clinical status are generally defined according to the World Health Organization guidelines.[1]
Moreover, malaria cases are designated as severe (complicated) cases
depending on certain laboratory (e.g. parasitemia > 5%, severe
normocytic anemia of Hb < 5g/dl, renal impairment where serum
creatinine > 265 µmol/l) and clinical (e.g. impaired consciousness
or coma, multiple convulsions, pulmonary edema) findings. Accordingly,
severe (complicated) malaria cases are admitted to the medical
intensive care unit (MICU) or the short stay unit, while uncomplicated
cases are managed in an outpatient setting. A variety of anti-malarial
medications are prescribed, such as: Patients diagnosed with
uncomplicated and complicated/severe P. falciparum
infection were treated with chloroquine and quinine plus doxycycline
(adults)/or clindamycin (children)/or artemether and lumefantrine
combination, respectively. Chloroquine, followed by primaquine is
recommended for patients with P. vivax malaria. Those with mixed infections are usually treated as P. falciparum malaria.
All
samples undergo screening for the malaria parasite through microscopic
examination with Giemsa staining of thin and/or thick blood films.
Furthermore, the malaria focal point of MoPH’s communicable disease
control section conducted the epidemiological investigation and
follow-up. All patients diagnosed with malaria were treated with
anti-malarial medication as per the current guidelines for malaria
treatment at HMC.
Results
A
total of 4092 malaria cases reported during 2008-2015 were analyzed to
describe the epidemiological features of imported malaria in the State
of Qatar, using demographic profiling through parameters such as age,
gender, nationality (either Qatari, or migrant expatriates who have
lived in Qatar for at least 1 year), travel history, time of malaria
reporting, and Plasmodium species.
All
cases were imported and underwent parasitological confirmation through
microscopy; where no relapses were reported. Additionally, all patients
received anti-malarial treatment with no accurate information about how
many people exactly received such treatment. Therefore, none of the
malaria patients were followed-up for 28 days. Furthermore, twelve
cases of complicated or severe malaria have been documented throughout
2014 and 2015, and one of them was fatal. The causative organisms in
more than half of such cases were P. falciparum (58.3%), followed by P. vivax (33.3 %), and mixed infection (8.3 %).
The
annual number of imported malaria cases in Qatar has nearly tripled
from 216 cases in 2008 to 728 cases in 2013. However, the number of
malaria cases has declined to reach 445 cases in 2015. The demographic
features of the imported cases (Table 1)
show that the majority of cases were males (93%), non-Qatari (99.6%),
and aged 15 to 44 years (82.1%). In addition, almost a third (33.1%) of
the cases were reported between July and September (Figure 1). Furthermore, between 2008-2009 and 2012-2015, P. vivax
was found to be the main etiologic agent accounting for more than
three-quarters (78.7%) of the cases. In addition, during the time above
period, P. falciparum was found to be responsible for almost one-seventh (13.6%) of the cases. However, data on the causative Plasmodium species during 2010 and 2011 were not recorded and thus are not reported in this study.
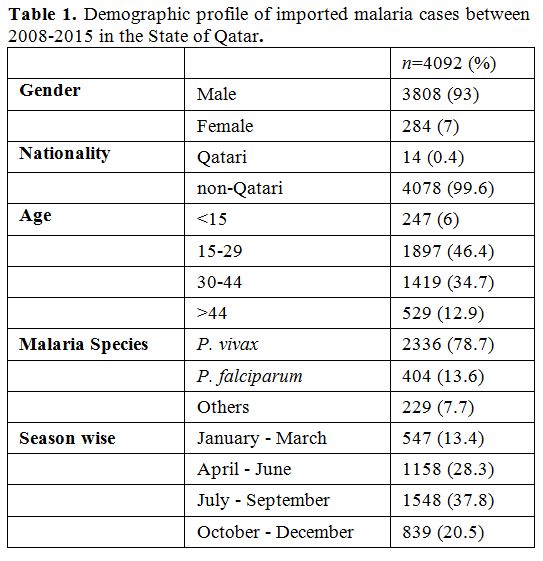 |
Table 1.
Demographic profile of imported malaria cases between 2008-2015 in the State of Qatar. |
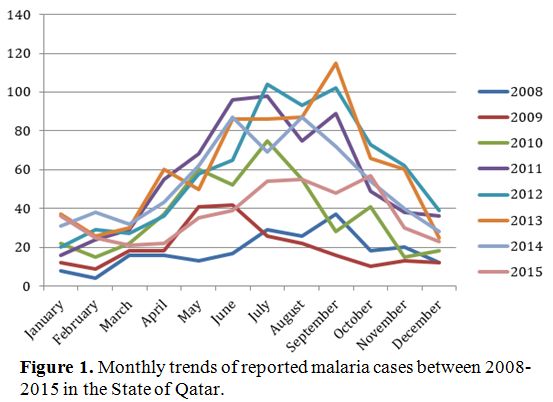 |
Figure 1. Monthly trends of reported malaria cases between 2008-2015 in the State of Qatar. |
A
total of 1,816 malaria cases were reported between 2013 and 2015 to the
surveillance section at the Ministry of Public Health, Qatar. After
further analysis, the regional distribution of the cases’ country of
origin revealed that almost half originated from the South East Asia
Region (44.7%) and the other half from the Eastern Mediterranean Region
(43.2%) (Table 2). The
distribution of malaria cases by nationality and country of origin
reveal that all cases have contracted the malarial infection from
patient’s country of origin and due to travel to endemic countries.
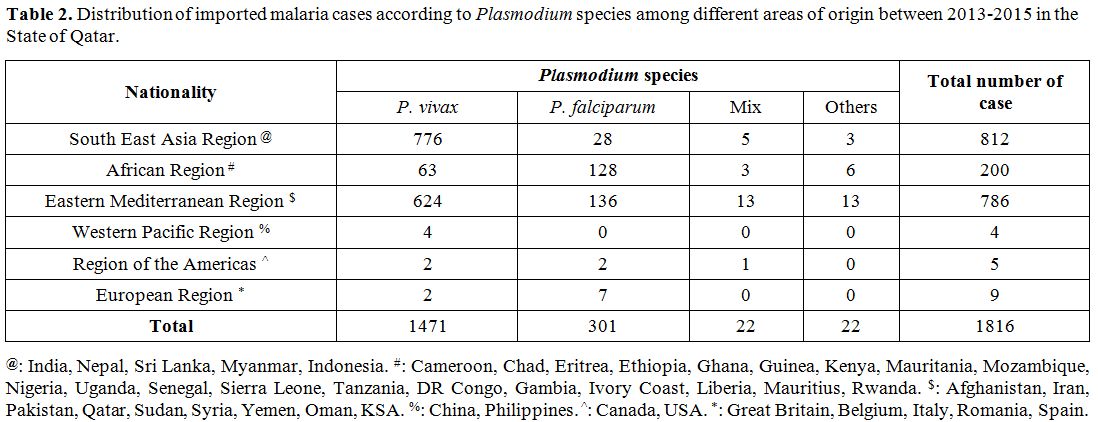 |
Table
2. Distribution of imported malaria cases according to Plasmodium
species among different areas of origin between 2013-2015 in the State
of Qatar. |
Discussion
Malaria
continues to be the most important vector-borne infectious disease and
a major health problem in South East Asia and Africa. One of the main
factors contributing to this sustained burden is the emergence and
spread of anti-malarial drug resistance as well as vector resistance to
insecticides.[10] In addition to that, increased
international travel and dramatic climate changes have disturbed the
conventional epidemiological pattern of endemic infectious diseases.
In the present study, the majority of cases were male, non-Qatari, presented at >15 years of age, P. vivax was the main etiologic agent and occurred between July and September; which corroborates with previous studies in Qatar[7,9] and those of neighboring Gulf countries.[11-13]
These data indicate that imported malaria in Qatar has shown an
increase after a long period of constant reduction, and most cases
occurred between July and September, which confirms that the infection
was imported from patients’ respected countries during the summer
vacation.[7,9] Furthermore, the
reason of higher malaria cases in the male gender and 25 years old age
group in the current study must be due to the massive influx of single
male expatriates as labor from malaria-endemic regions of South East
Asian Countries and African continents. This pattern has also been
reported from previous studies in the Gulf region and western
countries.[11,13-15]
The Gulf
Cooperation Council (GCC) countries have accomplished against malaria
control; however, the region has witnessed the influx of a large
immigrant workforce, which travels to and from the respective home
countries annually. Moreover, such labor force arises primarily from
the malaria-endemic countries of India, Pakistan, and Bangladesh.
Therefore, imported malaria can pose a significant threat to malaria
control programs and the prospect of elimination in some of GCC
countries, where transmission has been interrupted previously. In the
United Arab Emirates, almost 3239 cases of imported malaria were
identified; the majority of which (90%) originated from Pakistan and
India. On the other hand, the Kingdom of Saudi Arabia reported 1912
cases of imported malaria; almost a third of which (30%) originated
from neighboring Yemen. In addition to that, the majority (89%) of the
528 imported malaria cases in the Kingdom of Bahrain were among
nationals of India and Pakistan.[16]
It is well documented that mostly Indo-Gangetic plains, Northern hilly states, Northwestern and Southern India have < 10% P. falciparum, and the rest are P. vivax infections,[17] whereas, in African countries, P. falciparum is predominant.[6] In the present study, P. vivax was more commonly isolated in patients from India, Nepal, and Pakistan. On the other hand, P. falciparum
was more commonly found among patients from Sudan. These findings are
consistent with previous findings of research from neighboring Gulf
countries.[11-13,18,19]
In the
present study, our data clearly indicate that imported malaria in Qatar
has constantly increased from 2008 to 2013 and those most affected were
adult male migrants from endemic countries such as India, Nepal,
Pakistan, and Sudan. The increase in the total number of reported
imported malaria cases between the 2008 and 2015 could be explained by
the increased influx of foreign workers from malaria-endemic countries.
In 2015, WHO’s theme for World Malaria Day was “Invest in the Future:
Defeat Malaria”, which highlights the advances made in preventing,
controlling, and eliminating malaria globally. Consequently, to reduce
the importation of malaria cases into the State of Qatar, the Ministry
of Public Health (MoPH) held a public health awareness campaign
targeting all travelers to malaria-endemic countries. Moreover, the
ministry provides free malaria prophylaxis in travel clinics, which
could explain the decline of malaria incidence during 2014-2015 in
Qatar.
Imported malaria in Qatar has witnessed an increase
during the past seven years, despite a long period of constant
reduction; where the people most affected were adult male migrants from
endemic countries. Additionally, challenges as a weak malaria
surveillance system, lack of malaria awareness among health
professionals as well as travelers, and a lack of cooperation among
stakeholders must be mitigated to prevent malaria reintroduction in the
country. With infrastructure expansions and new development in Qatar as
the country prepares to host the FIFA World Cup soccer tournament in
2022, it is expected that there will be a large influx of tourists,
foreign workers, and those visiting friends and relatives. Therefore,
the incidence of cases and the risk of malaria reintroduction are also
likely to increase. Thus, an enhanced and robust surveillance program
should be implemented to reduce imported malaria cases in the State of
Qatar.
Acknowledgments
We
would like to acknowledge Mr. Redentor Cuizon Ramiscal, the
nurse-in-charge of the malaria notification forms and the surveillance
section under the Public Health Department at the Ministry of Public
Health, for his kind support and facilitation of our study.
References
- World Health Organization. World malaria report 2017. Geneva: WHO Press; 2017.

- Fact Sheet: World Malaria Report 2015 [Internet]. who.int. 2016 [cited 15 March 2018]. Available from: http://www.who.int/malaria/media/world-malaria-report-2015/en/
- Committee on Malaria Vaccines. Vaccines against malaria. 1st ed. Washington, D.C.: National Academies Press; 1996.
- Smith
A, Bradley D, Smith V, Blaze M, Behrens R, Chiodini P et al. Imported
malaria and high risk groups: observational study using UK surveillance
data 1987-2006. BMJ. 2008;337(jul03 2):a120-a120.
- Franco-Paredes
C, Santos-Preciado JI. (2006) Problem pathogens: prevention of malaria
in travellers. Lancet Infect Dis. 6 (3): 139-149. https://doi.org/10.1016/S1473-3099(06)70410-8
- Beljaev A. The malaria situation in the WHO eastern Mediterranean region. Meditsinskaia Parazitologiia. 2000;(2):12-5.
- Al-Kuwari M. Epidemiology of Imported Malaria in Qatar. Journal of Travel Medicine. 2009;16(2):119-122. https://doi.org/10.1111/j.1708-8305.2008.00285.x PMid:19335812
- Qatar - International tourism [Internet]. Indexmundi.com. [cited 15 March 2018]. Available from: http://www.indexmundi.com/facts/qatar/international-tourism
- Khan
F, Lutof A, Yassin M, Khattab M, Saleh M, Rezeq H et al. Imported
malaria in Qatar: A one year hospital-based study in 2005. Travel
Medicine and Infectious Disease. 2009;7(2):111-117. https://doi.org/10.1016/j.tmaid.2009.01.003 PMid:19237144
- Status report on artemisinin and ACT resistance (April 2017) [Internet]. who.int. 2017 [cited 15 March 2017]. Available from: http://www.who.int/malaria/publications/atoz/9789241500479/en/index.html
- Iqbal J, Al-Ali F, Sher A, Hira P. Imported Malaria in Kuwait (1985-2000). Journal of Travel Medicine. 2003;10(6):324-329. https://doi.org/10.2310/7060.2003.9291 PMid:14642198
- Ismaeel
AY, Senok AC, Jassim Al-Khaja KA, Botta GA . Status of malaria in the
Kingdom of Bahrain: a 10-year review. J Travel Med 2004; 11: 97 – 101. https://doi.org/10.2310/7060.2004.17059 PMid:15109474
- Bashwari
L, Mandil A, Bahnassy A, Al-Shamsi M, Bukhari H. Epidemiological
profile of malaria in a university hospital in the eastern region of
Saudi Arabia. Saudi Medical Journal. 2001;22(2):133-8. PMid:11299407
- Dar
F, Bayoumi R, AlKarmi T, Shalabi A, Beidas F, Hussein M. Status of
imported malaria in a control zone of the United Arab Emirates
bordering an area of unstable malaria. Transactions of the Royal
Society of Tropical Medicine and Hygiene. 1993;87(6):617-619. https://doi.org/10.1016/0035-9203(93)90261-N
- Lobel
H, Baker M, Gras F, Stennies G, Meerburg P, Hiemstra E et al. Use of
Malaria Prevention Measures by North American and European Travelers to
East Africa. Journal of Travel Medicine. 2001;8(4):167-172. https://doi.org/10.2310/7060.2001.22206 PMid:11703900
- Snow
R, Amratia P, Zamani G, Mundia C, Noor A, Memish Z et al. The Malaria
Transition on the Arabian Peninsula: Progress toward a Malaria-Free
Region between 1960–2010. Advances in parasitology. 2013;82:205–251. https://doi.org/10.1016/B978-0-12-407706-5.00003-4 PMid:23548086 PMCid:PMC3951717
- Kumar
A, Valecha N, Jain T, Dash A. Burden of malaria in India: retrospective
and prospective view. American Journal of Tropical Medicine and
Hygiene. 2007;77(6):69-78. PMid:18165477
- Al-Seghayer
SM, Kenawy MA, Ali OTE . Malaria in the Kingdom of Saudi Arabia
epidemiology and control . Sci J King Faisal University 1999; 1: 6 –
20.
- Al-Tawfiq
J. Epidemiology of travel-related malaria in a non-malarious area in
Saudi Arabia. Saudi Medical Journal. 2006;27(1):86-9. PMid:16432601
[TOP]