Annamaria Tomasso1, Idanna Innocenti2, Francesco Autore2, Alberto Fresa1, Giulia Benintende1, Florenzia Vuono1, Silvia Baroni3, Claudia Giannotta4, Patrizia Chiusolo1,2, Federica Sorà1,2, Simona Sica1,2 and Luca Laurenti1,2.
1
Sezione di Ematologia, Dipartimento di Scienze Radiologiche ed Ematologiche, Università Cattolica del Sacro Cuore, Rome, Italy.
2
Dipartimento di Diagnostica per Immagini, Radioterapia Oncologica ed
Ematologia, Fondazione Policlinico Universitario A. Gemelli IRCCS,
Rome, Italy.
3 Dipartimento di Chimica Clinica,
Fondazione Policlinico Universitario A. Gemelli IRCCS, Università
Cattolica del Sacro Cuore, Roma, Italy.
4 Department
of Medical Biotechnology and Translational Medicine, Milan University,
Neuromuscular and Neuroimmunology Service, Humanitas Clinical and
Research Center, Rozzano, Italy.
Correspondence to:
Luca Laurenti MD, Largo A. Gemelli 8, 00168 Rome, Italy. Tel:
39-06-30156016. Fax: 39-06-3017319. E-mail:
luca.laurenti@unicatt.it
Published: January 1, 2022
Received: September 16, 2021
Accepted: December 8, 2021
Mediterr J Hematol Infect Dis 2022, 14(1): e2022007 DOI
10.4084/MJHID.2022.007
This is an Open Access article distributed
under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by-nc/4.0),
which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
|
To the editor
POEMS is a paraneoplastic syndrome due to an underlying plasma cell neoplasm[1]
characterized by polyneuropathy, organomegaly, endocrinopathy,
M-protein accumulation, and skin changes, even if not all necessarily
present in the same patient at the same time.
VEGF function may be responsible for most of POEMS manifestations,[2]
and it is considered a reliable marker of disease, used for both
diagnosis and follow-up, as it correlates well with disease status.
However, the shortage of centers performing ELISA testing for VEGF
poses the need to look for more largely available markers for POEMS
diagnosis and follow-up.
COVID-19 era arose increasing interest
for inflammatory cytokines, with particular focus on Interleukin-6
(IL-6): therefore, many laboratories developed and strengthened the
analysis of its level in the blood, which, at the same time, opened us
a window of opportunity for further investigation in the field of POEMS
physiopathology and surveillance.
Recently, inflammatory
pathways have gained considerable interest as an important mediator of
the molecular mechanisms leading to hematological malignancies. VEGF
production is stimulated by the cytokines IL-6 and IL1β, whose
concentrations appear to be elevated in clonal plasma cell diseases.[3]
Previous studies have found chronically elevated serum IL-6 in patients
(patients) diagnosed with POEMS syndrome, compared to patients
diagnosed with other clonal disorders, which points out a possible role
of IL-6 function in POEMS development.[4] Case reports
have also investigated the presence of IL-6 in some of the involved
organs, finding even higher levels in pericardial effusion,[5] ascites,[6] and renal glomeruli[7] compared to serum.
Even if the role of IL-6 as a marker of disease activity is largely recognized,[8]
so far, there is no proof of any correlation between serum levels of
VEGF and IL-6. Nevertheless, their dosage at various stages of the
disease, particularly in the peri-transplant period, aims to understand
if they have a comparable pattern, and therefore IL-6 could be used in
clinical practice for disease monitoring.
Materials and Methods.
In
the present analysis, performed as a monocentric study at "Policlinico
Gemelli" in Rome, we measured circulating levels of VEGF and IL-6 in 8
patients diagnosed with POEMS. Three of them have been studied before
and after eradicating therapy with Melphalan 200 mg/mq followed by
autologous BMT, particularly the day after the infusion and after one
month, so that data are available for both periods. Four of them have
been periodically examined for a long period, only later after
transplant, each at multiple time points over two to 17 years after
BMT, so that late-stage data are available. Furthermore, we analyzed a
newly diagnosed POEMS patient and detected his baseline assessment of
serum VEGF and IL-6.
Cytokine profiles were determined on serum
samples using Immunoassay panels (i.e., anti-IL-6 and anti-VEFG ELISA
kit). Detection of cytokines and growth factors was performed per the
manufacturer's instruction.
Results
The first three patients, observed before transplant, presented with
elevated serum levels of both VEGF and IL-6 since they were on active
disease. The measurement performed the day after the infusion of
autologous stem cells, instead, showed a steep decrease of both serum
markers, likely due to the pre-transplant conditioning regimen,
followed by a modest increase in the late post-transplant phase (Figure 1a).
In
the group of four patients tested only after the transplant, one
patient was observed at three-time points every four months starting
two years after transplantation and presented with steady normal IL-6
values over the time despite a significantly elevated VEGF (Figure 1b);
another patient was observed twice with a one-year time span starting
two years after transplantation and presented with elevated IL-6, but
decreasing until it became normal, despite a stable normal value of
VEGF (Figure 1c); the last two
patients were observed annually twice, in the late post-BMT phase
(i.e., starting 5 and 16 years after BMT, respectively) and a
correlation between the two values was detected, being both within the
normal range (Figure 1d and 1e).
Regarding
the patient who was observed just at diagnosis, thus on active disease,
his baseline assessment showed strikingly high levels of both serum
VEGF (5,6 ng/mL, with normal values < 1 ng/mL) and IL-6 (21,6 pg/mL,
with normal values < 4,4 pg/mL).
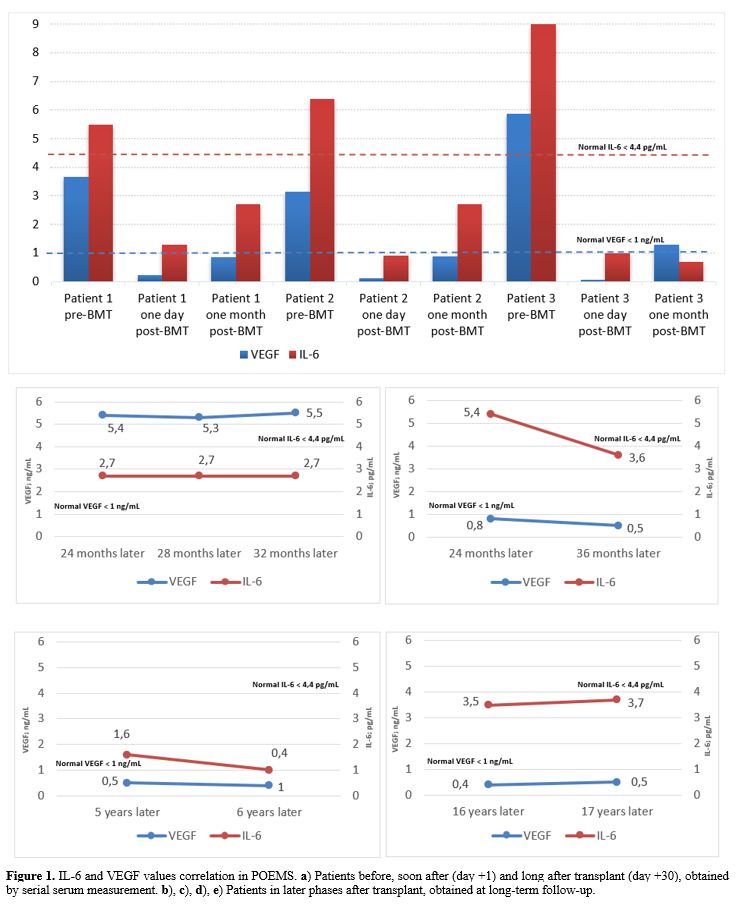 |
Figure
1. IL-6 and VEGF values correlation in POEMS. a) Patients before, soon
after (day +1) and long after transplant (day +30), obtained by serial
serum measurement. b), c), d), e) Patients in later phases after
transplant, obtained at long-term follow-up.
|
Discussion
The
patients studied before and after transplant showed concordance in the
values of VEGF and IL-6 at the three different time points; the
decrease immediately after the stem cells infusion is probably
explained by the sharp therapeutic effect of eradicating regimen, which
constitutes the only curative treatment for POEMS nowadays and is
therefore used as frontline therapy.[9] Furthermore,
the pattern of the two markers displayed some similarities; thus, it
could eventually be asserted that the two values correlate in the
peri-transplant phase of the disease.
Alternatively, the other
four patients showed variable VEGF and IL-6 serum levels, which only
correlate in two patients in complete remission after the autologous
BMT transplantation and who had no comorbidities. Normal IL-6 but
elevated VEGF detected in the fourth patient could be justified by a
relapsed active disease after many lines of treatment, including
autologous BMT, even if the mechanism underlying this lack of
concordance remains unclear. The swinging values of IL-6 compared to
normal values of VEGF of the other patient in this group could be due
to the secondary development of multicentric Castleman disease (MCD),[10]
whose pathogenesis is known to be driven by IL-6 in some patients and
to increase the overall cytokine levels by itself, regardless of the
concomitant presence of POEMS. However, how the cellular and cytokine
profiles between POEMS-MCD and classic POEMS syndrome differ is
unknown.[11] Thus, the two markers should be considered separately as markers of two distinct diseases in this patient.
Furthermore,
the concordance between the baseline values of serum VEGF and IL-6 at a
stage of severe and active disease detected in the last patient could
suggest that IL-6 may be a reliable marker of disease burden.
In
conclusion, further patients' analysis should be prompted to confirm an
existing relation between VEGF and IL-6: the use of IL-6 as a marker of
disease would allow easier monitoring of the disease status,
particularly regarding the active phase of the disease and the
peri-transplant period. However, there is no sufficient evidence about
IL-6 behavior at later stages or long follow-up in post-transplant
patients. Moreover, several confounding factors, such as the occurrence
of comorbidities or Castleman disease, could alter the IL-6 values,
independently of POEMS status.
So far, to the best of our
knowledge, IL-6 could be considered reliable up to the very first
months after BMT, after which its accuracy appears to be lost due to
unknown factors, still to be investigated.
References
- Dispenzieri A. POEMS Syndrome: 2019 Update on
diagnosis, risk-stratification, and management. Am J Hematol. 2019
Jul;94(7):812-827. https://doi.org/10.1002/ajh.25495 PMid:31012139
- Soubrier
M, Dubost JJ, Serre AF, et al. Growth factors in POEMS syndrome:
evidence for a marked increase in circulating vascular endothelial
growth factor. Arthritis Rheum. 1997 Apr;40(4):786-7. https://doi.org/10.1002/art.1780400430 PMid:9125266
- Tzeng
HE, Tsai CH, Chang ZL, et al. Interleukin-6 induces vascular
endothelial growth factor expression and promotes angiogenesis through
apoptosis signal-regulating kinase 1 in human osteosarcoma. Biochem
Pharmacol. 2013;85(4):531-540. https://doi.org/10.1016/j.bcp.2012.11.021 PMid:23219526
- Gherardi
RK, Bélec L, Fromont G, et al. Elevated levels of interleukin-1 beta
(IL-1 beta) and IL-6 in serum and increased production of IL-1 beta
mRNA in lymph nodes of patients with polyneuropathy, organomegaly,
endocrinopathy, M protein, and skin changes (POEMS) syndrome. Blood.
1994;83(9):2587-2593. https://doi.org/10.1182/blood.V83.9.2587.2587 PMid:8167341
- Fukatsu
A, Ito Y, Yuzawa Y, et al. A case of POEMS syndrome showing elevated
serum interleukin 6 and abnormal expression of interleukin 6 in the
kidney. Nephron. 1992;62(1):47-51. https://doi.org/10.1159/000186994 PMid:1436291
- Minamitani
S, Ohfuji S, Nishiguchi S, et al. An autopsy case of POEMS syndrome
with a high level of IL-6 and VEGF in the serum and ascitic fluid.
Intern Med. 2002;41(3):233-236. https://doi.org/10.2169/internalmedicine.41.233 PMid:11929188
- Fukatsu
A, Ito Y, Yuzawa Y, et al. A case of POEMS syndrome showing elevated
serum interleukin 6 and abnormal expression of interleukin 6 in the
kidney. Nephron. 1992;62(1):47-51. https://doi.org/10.1159/000186994 PMid:1436291
- Hitoshi
S, Suzuki K, Sakuta M. Elevated serum interleukin-6 in POEMS syndrome
reflects the activity of the disease. Intern Med. 1994;33(10):583-587. https://doi.org/10.2169/internalmedicine.33.583 PMid:7827372
- Laurenti
L, De Matteis S, Sabatelli M, et al. Early diagnosis followed by
frontline autologous peripheral blood stem cell transplantation for
patients affected by POEMS syndrome. Leuk Res. 2008 Aug;32(8):1309-12. https://doi.org/10.1016/j.leukres.2007.11.029 PMid:18207237
- Yoshizaki
K, Murayama S, Ito H, Koga T. The Role of Interleukin-6 in Castleman
Disease. Hematol Oncol Clin North Am. 2018;32(1):23-36. https://doi.org/10.1016/j.hoc.2017.09.003 PMid:29157617
- Dispenzieri A, Fajgenbaum DC. Overview of Castleman disease. Blood 2020; 135 (16): 1353-1364. https://doi.org/10.1182/blood.2019000931 PMid:32106302
[TOP]