Background:
The paper was to investigate the clinical relevance of oxidative stress
(OS) and inflammation-associated targets in coronary artery lesions
(CALs) associated with Kawasaki disease (KD).
Methods:
The clinical data from 455 sufferers diagnosed with KD between February
2021 and June 2023 were gathered and divided into two groups: CAL and
NCAL. The regression analysis was conducted to search for independent
covariates for CALs related to OS and inflammation. The predictive
nomogram was structured according to these risk factors. The properties
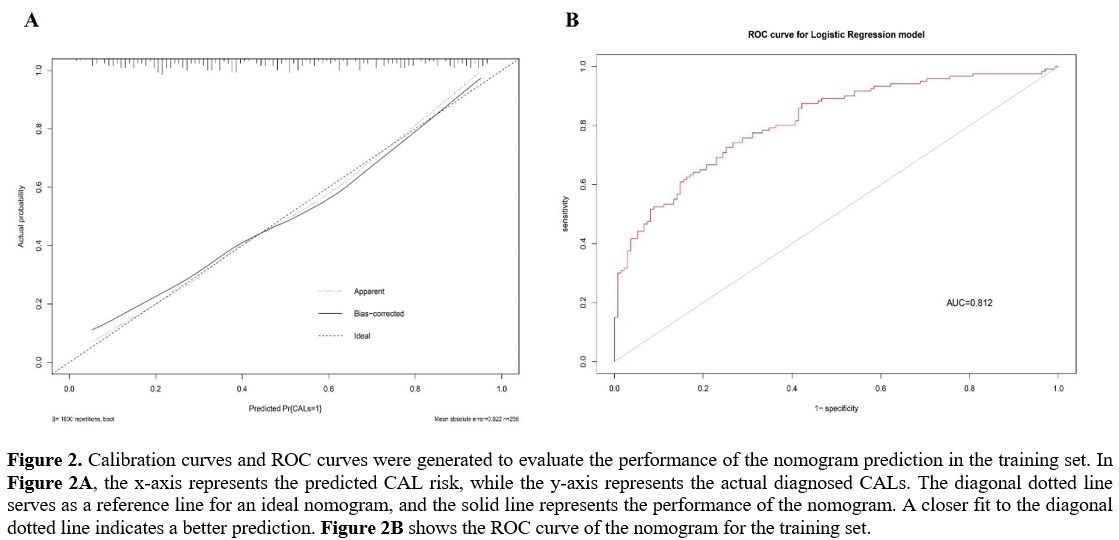
of the model were estimated using calibration and receiver operating
characteristic curves.
Results:
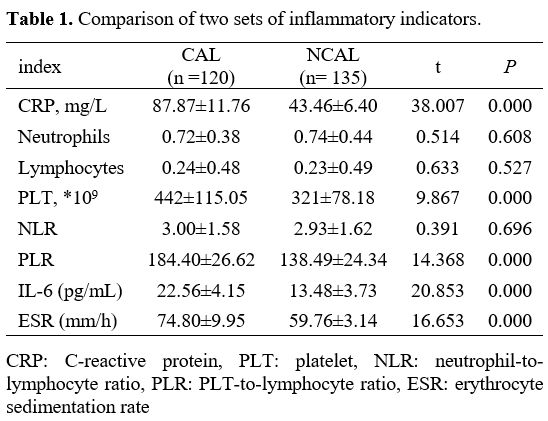
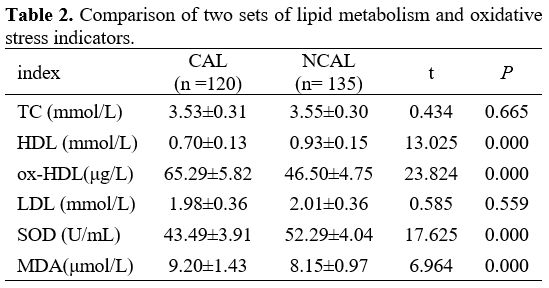
The levels of CRP, IL-6, PLT count, ESR, ox-HDL, MDA, and PLR were more
elevated in CAL patients with KD; interestingly, HDL and superoxide
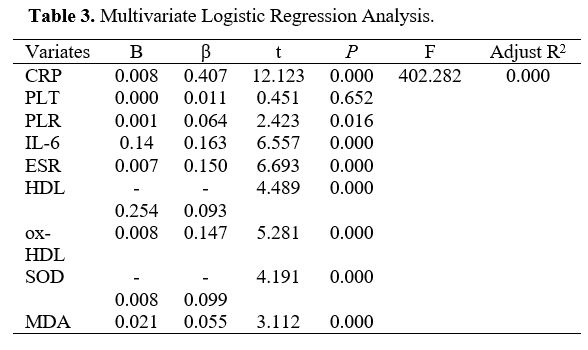
dismutase (SOD) were low in the CAL group. Ascension of CRP, IL-6, ESR,
ox-HDL, MDA, and PLR, and diminution of HDL and SOD were considered
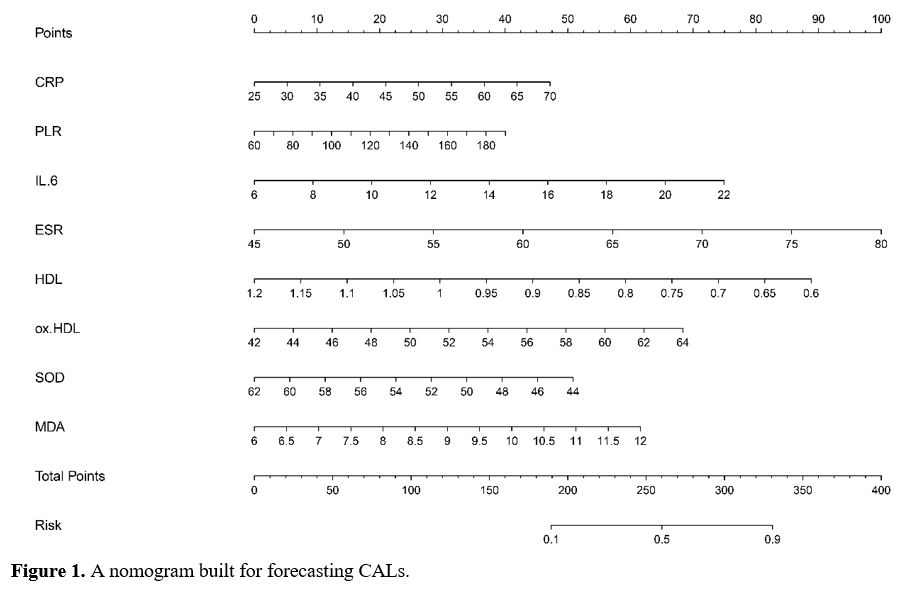
independent risk factors. The nomogram constructed using these factors
demonstrated a satisfactory calibration degree and discriminatory
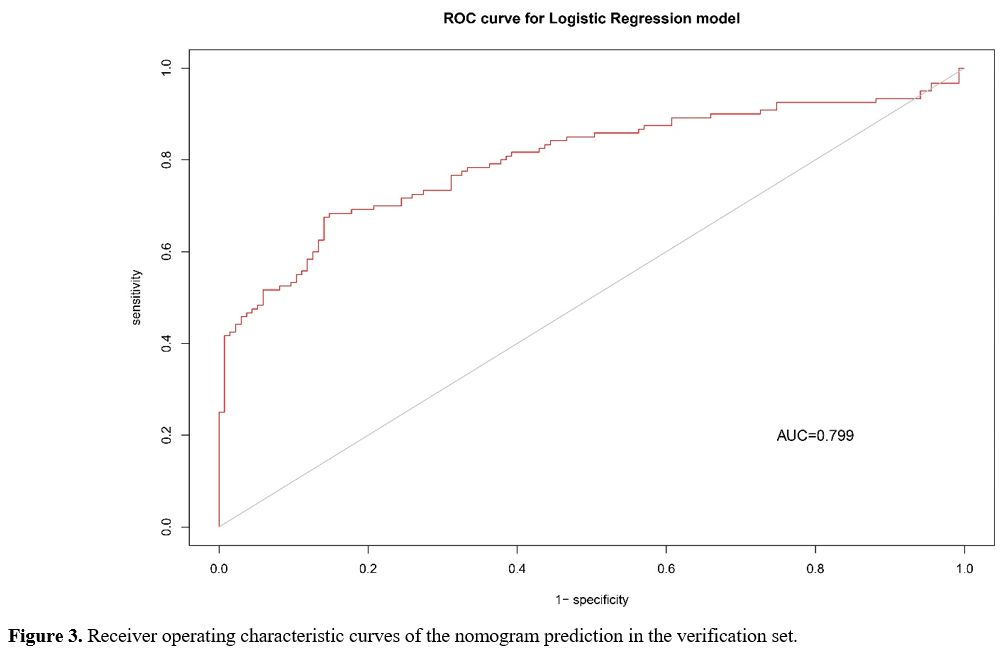
power, with an area under the curve of 0.812. In the verification set,
the area under the curve was found to be 0.799.
Conclusion:
The model was established according to 8 OS and inflammation-associated
risk factors bound up with CALs in KD sufferers. It may be a usable
approach for early diagnosis of CALs in KD.