A three-year-old boy with severe thrombocytopenia, mild macrocytic anemia, leukopenia, and 12% myeloid peripheral blasts was admitted at Instituto de Pediatria e Puericultura Martagão Gesteira, Universidade Federal do Rio de Janeiro, Brazil, in January 2016. Bone marrow (BM) evaluation evidenced marked erythroid dysplasia, megakaryocytic dysplasia, and 14% of myeloid blasts. Cytogenetic analysis of BM cells by G-banding revealed the complex karyotype: 49, XY, del(3)(q21), del(6)(q21),+der(6)del(6)(q21),+8,+der(12)del(12)(p11)[21] (Figure 1A). FISH analysis confirmed the +8 (Figure 1B). The patient was diagnosed with MDS with increased blasts (MDS-IB).[5] Next-generation sequencing (NGS) analysis using the Ion Torrent Personal Genome Machine (PGM) platform (Life Technologies) was performed for the genes: GATA2, RUNX1, CEBPA, ANKRD26, ETV6, SAMD9, SAMD9L, PTPN11, NRAS, SETBP1, DDX41, TP53, FLT3, SRP72 and JAK3. An ETV6 likely pathogenic variant was identified, with the molecular consequence of the loss of the termination codon (stop-loss variant) (Table 1). He evolved with worsening cytopenias, transfusion requirements, and progression to MDS/AML. He was treated with thioguanine but he did not show response to this treatment. More intensive chemotherapy was performed for induction of minimal residual disease (MRD); then, he was referred to Bone Marrow Transplantation Center, Instituto Nacional de Cancer, and underwent allo-HSCT from his nine years old female HLA-matched sibling donor, with minor ABO incompatibility. The myeloablative conditioning regimen consisted of busulfan/cyclophosphamide (BU/CY) and graft-versus-host disease (GVHD) prophylaxis of methotrexate (MTX) and cyclosporine (CSA). The engraftment occurred on D+21. BM evaluation at D+45 post-transplant showed negative MRD by flow cytometry, donor karyotype 46, XX[35], and mixed donor chimerism by PCR short tandem repeats (STR) analysis (96.9% in mononuclear cells and 100% in granulocytic population). However, at D+75, peripheral blood and BM analysis revealed pancytopenia, myeloid dysplasia, and a decline in donor chimerism to 87.5% in the mononuclear population. Attempts to carry out preemptive donor lymphocyte infusions (DLIs) did not materialize because the donor had recurrent respiratory infections at that time. The patient received one cycle of azacitidine (AZA) with improvement of hepatomegaly, bone pain, and hematological counts, but soon after, he evolved with severe thrombocytopenia and respiratory infection. At D16 of AZA, the patient showed 2% of blasts compatible with megaloblasts and 12% of dysplastic megakaryocytic lineage by flow cytometry. His clinical condition worsened around D+137, with aggravation of pancytopenia due to a progressive decrease in donor chimerism (47.8% in the mononuclear population). At that point, flow cytometry showed 18% of dysplasia in the megakaryocytic sector. Overt disease relapse occurred at D+180 post-HSCT. The cytogenetic analysis showed the CCE: 50, XY, del(3)(q21),+der(3)del(3)(q21), del(6)(q21),+der(6) del(6)(q21),+8,+der(12)del(12)(p11)[2]/46, XX[19] (Figure 1C). The patient had 14.2% of positive cells for +8 by FISH (Figure 1D). The immunophenotyping showed 5% of blasts, and STR detected mixed donor chimerism in both lineages (59.9% mononuclear and 77.3% in granulocytic populations). Salvage chemotherapy with fludarabine plus cytarabine and idarubicin was started. Despite attempts to control the disease, it progressed; the patient developed severe persistent pancytopenia (with transfusion dependency) and massive pulmonary aspergillosis that led to his death after 8 months post-HSCT.
 |
Figure 1. Conventional and molecular cytogenetics of BM cells in pediatric MDS at diagnosis and post-HSCT. (A)
G-banding showing the complex karyotype:
49,XY,del(3)(q21),del(6)(q21),+der(6)del(6)(q21),+8,+der(12)del(12)(p11);
(B) FISH analysis using the c-MYC probe (LSI MYC spectrum orange, 8q24, Vysis) showing trisomy 8 (three red signals); (C)
G-banding analysis post-HSCT showing a cytogenetic clonal evolution:
50,XY,del(3)(q21),+der(3)del(3)(q21),del(6)(q21),+der(6)del(6)(q21),+8,+der(12)del(12)(p11);
(D) FISH analysis using the
c-MYC probe (LSI MYC spectrum orange, 8q24, Vysis) showing cells with
trisomy 8 and normal cells (two red signals). |
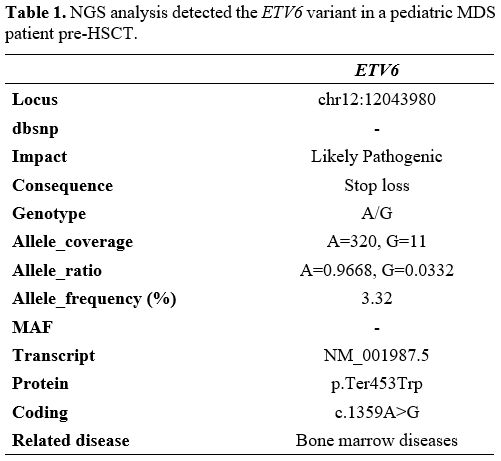 |
Table 1. NGS analysis detected the ETV6 variant in a pediatric MDS patient pre-HSCT. |
The complex karyotype is a cytogenetic biomarker indicative of poor survival after HSCT in MDS patients.[4] The MDS genetic diversity amongst coexisting subclones may result in a more heterogeneous and complex disease, as some of the subclones may be resistant to specific types of therapy.[6] In the present report, the patient pre-HSCT had a complex karyotype. Post-HSCT, the patient showed disease relapse and CCE, represented by the acquisition of a der(3)del(3)(q21). The del(3)(q21) involves the loss of important genes such as GATA2,[7] BCL6[8] and MECOM.[9] The del(3q) was also present at the abnormal cytogenetic clone detected at diagnosis with other chromosomal abnormalities involving important genes such as MYB in del(6)(q21); c-MYC in +8; and ETV6 in del(12)(p11). It is interesting to note the high genomic instability in this patient, who also acquired the gain of these abnormal chromosomes, resulting in chromosome derivatives. These extra copies can lead to overexpression of important genes mapped to these chromosome regions as FANCD2, RASSF1 in 3p; DEK, CDKN1A in 6p, and WNT1, HOXC13 in 12q.[8] ETV6 is subject to heterozygous mutations in hematologic malignancies, including MDS. ETV6 is a major intrinsic regulator of megakaryocytes.[10,11] Besides that, ETV6 is one of the key regulators of sepsis, a major cause of morbidity and mortality in the intensive care unit.[12] In this case, the complex karyotype and the loss of heterozygosity in ETV6 (chromosomal deletion and genetic variant) may be associated with disease relapse and unfavorable clinical outcome post-transplant. Ertz-Archambault and colleagues observed cytogenetic evolution in myeloid neoplasms in adult patients who had disease recurrence after HSCT. The authors observed that an unfavorable cytogenetic profile at the initial diagnosis may represent an important pre-diagnosis factor of a predisposition for clonal evolution. The acquisition of more complex cytogenetic alterations is associated with lower survival.[6] Our study suggests that the treatment of MDS patients with predictive factors of poor prognosis, such as complex karyotypes and ETV6 variant, remains a challenge. Prospective studies are necessary to characterize the biology of MDS and identify molecular biomarkers associated with disease relapse in order to develop precision medicine to improve the survival of this group of patients.